Lietuvos chirurgija ISSN 1392–0995 eISSN 1648–9942
2023, vol. 22(3), pp. 158–160 DOI: https://doi.org/10.15388/LietChirur.2023.22(3).4
Portal Vein and Superior Mesenteric Vein Invasion of Hydatid Cyst of The Liver: Surgical Treatment Option
Ali Sapmaz
Department of General Surgery, Ankara Bilkent City Hospital, University of Health Sciences, Ankara, Turkey
E-mail: alisapmaz@gmail.com
Egemen Cicek
Department of General Surgery, Faculty of Medicine, İnönü University, Malatya, Turkey
E-mail: egemen.cicek@gmail.com
Serhan Yilmaz
Department of General Surgery, Istanbul Kanuni Sultan Suleyman Training and Research Hospital, University of Health Sciences, Istanbul, Turkey
E-mail: drserhanyilmaz@gmail.com
Hakan Bolukbasi
Department of General Surgery, Istanbul Kanuni Sultan Suleyman Training and Research Hospital, University of Health Sciences, Istanbul, Turkey
E-mail: hbbolukbasi@gmail.com
Ahmet Soykurt
Department of General Surgery, Near East University Hospital, Nicosia, Cyprus
E-mail: ahmet.soykurt@gmail.com
Selcuk Mevlut Hazinedaroglu
Department of General Surgery, Faculty of Medicine, Ankara University, Ankara, Turkey
E-mail: smhasinedaroglu@gmail.com
Abstract. Hydatid cyst is a parasitic infestation by a tapeworm of the genus Echinococcus granulosus which can be localized in all vascularized tissues and causes cystic lesions. We present a case of hydatid liver cyst with portal vein and superior mesenteric artery invasion. Hydatid cysts are still commonly seen in Turkey. We believe that the most efficacious and least morbid treatment alternative for such rare complications of hydatid cysts is surgery.
Key words: liver, hydatid cyst, portal vein, superior mesenteric artery.
Hidatidinė kepenų cista ir vartų venos bei viršutinės pasaito arterijos: chirurginio gydymo galimybė
Santrauka. Turkijoje vis dar dažnos hidatidinės cistos. Tai parazito Echinococcus granulosus klinikinė manifestacija, kuri lokalizuojasi visuose vaskuliarizuotuose audiniuose ir sukelia cistinius darinius. Straipsnyje aptariamas hidatidinės kepenų cistos atvejis, apimantis kepenų vartų veną ir viršutinę pasaito arteriją. Daroma išvada, kad efektyviausias ir mažiausiai komplikacijų sukeliantis šios retos patologijos gydymas yra chirurgija.
Reikšminiai žodžiai: kepenys, hidatidinė cista, vartų vena, viršutinė pasaito arterija.
Received: 2023/01/26. Accepted: 2023/03/14.
Copyright © 2023 Ali Sapmaz, Egemen Cicek, Serhan Yilmaz, Hakan Bolukbasi, Ahmet Soykurt, Selcuk Mevlut Hazinedaroglu. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution Licence, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Hydatid cyst is a parasitic infestation by a tapeworm of the genus Echinococcus granulosus which can be localized in all vascularized tissues and causes cystic lesions. The most common infection cites of hydatid cyst are liver (55–70%) and lung (18–35%). These two organs can be infected simultaneously in 5–13% of cases [1, 2]. On the other hand, atypical manifestation cites such as skin, central nervous system, retroperitoneum and breast can be detected. The prevalence of hydatid cyst is 2–6% in the endemic regions and it is considered as an important public health issue. The disease is mostly asymptomatic; however, it can be presented with abdominal mass, pain, fever and anaphylaxis. At the time of the diagnosis, 36–40% of the cysts are ruptured or infected. The disease generally affects the right lobe of the liver and it may cause upper-right abdominal pain, nausea and vomiting, when the cysts exceed 10 cm.
We report a hydatid cyst case in which the cyst invaded portal and superior mesenteric vein and caused thrombosis. The surgical approach is also discussed.
Case
A 53 year old male patient presented with severe abdominal pain. The patient had been operated 3 times for liver hydatid cyst due to Echinococcus granulosus. The ultrasonography demonstrated no portal blood flow and portal vein thrombosis was detected. There were vesicular cystic lesions inside the portal vein. Dynamic computerized tomography of the liver revealed lesions initiating from periportal region and extending to both liver lobes, which were associated with the hydatid cyst (Figure 1).
Moreover, the thrombus of echinococcus was extending until the lumen of superior mesenteric vein.
There were numerous hydatid cysts in the liver. There were a lot of portal collaterals in the portal hilus because of the hydatid thrombus inside the portal vein. Right and mid hepatic veins could not be visualized due to the thrombosis.
The patient underwent surgery and the hydatid cysts located in the right lobe of the liver were unroofed and the inner surface was rinsed with savlon solution. Afterwards, anterior and posterior parts of the left portal vein were examined. The parenchyma of the liver was incised and thrombotic right and middle hepatic veins were ligated. Right hepatectomy was performed over caval vein. The lumen of the portal vein was opened and no portal blood flow was seen (Figure 2).

Figure 1. CT scan
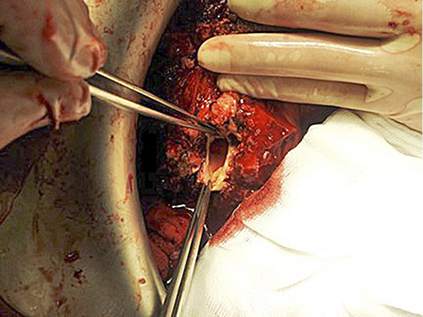
Figure 2. Thrombosed portal vein
The portal vein was catheterized and excessive amount of sister vesicles came out after the irrigation. However, no blood flow was detected with Doppler evaluation. The wall of the portal vein is repaired and other cystic lesions inside the liver parenchyma were emptied.
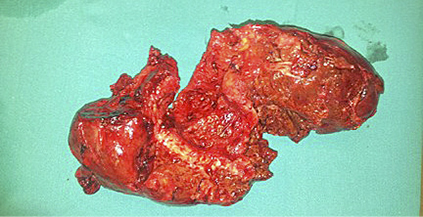
Figure 3. Pathology specimen
Discussion
The Echinococcus granulosus infection is endemically seen among people working with cows and lamps [3, 4]. The hydatid cyst is commonly localized in liver and lung; however, it can also infect brain, heart, kidney, ureter, spleen, uterus, fallopian tubes, mesentery, pancreas, diaphragm and striated muscle. Although percutaneous drainage and medical therapy are being used, surgical treatment is still considered as the gold standard.
In the literature, there are only a few hydatid cyst cases with thrombosis due to the the compression by the cyst or portal vein invasion. However, to our knowledge, there is not any reported case with vesicular appearance in the portal or mesenteric vein. The management of this extremely rare clinical entity is debatable. Non-surgical approaches such as ERCP have been used in the treatment of few cases. ERCP can have a limited benefit in cases with biliary tract involvement. The surgical treatment must be the treatment of choice in such cases. The cysts have been entirely removed without any detrimental effect on the collateral circulation and the vesicles inside the portal and mesenteric vein have been completely removed in our case. Portal and superior mesenteric vein were not re-canalized and the vascular structures were closed.
Hydatid cysts are still commonly seen in Turkey. We believe that the most efficacious and least morbid treatment alternative for such rare complications of hydatid cysts is surgery.
References
1. Kir A, Baran E. Simultaneous Operation for Hydatid Cyst of Right Lung and Liver. Thorac Cardiovasc Surg 1995; 43(1): 62–64.
2. Guntz M, Coppo B, Lorimier G, Cronier P. Hydatid Cyst of the Liver Appearing Late (10 to 22 Years) After Surgical Treatment of Pulmonary Hydatidosis. Physiopathologic Problems. J Chir (Paris) 1990; 127(8–9): 375–381.
3. Abu-Eshy SA. Some Rare Presentations of Hydatid Cyst (Echinococcus granulosus). J R Coll Surg Edinb 1998; 43(5): 347–352.
4. Brown RA, Millar AJ, Steiner Z, Krige JE, Burkimsher D, Cywes S. Hydatid Cyst of the Pancreas – a Case Report in a Child. Eur J Pediatr Surg 1995; 5(2): 121–123.