Psichologija ISSN 1392-0359 eISSN 2345-0061
2020, vol. 61, pp. 33–50 DOI: https://doi.org/10.15388/Psichol.2020.14
Factors Associated with Depression in Middle-Aged and Elderly People in Romania
Cornelia Rada
Biomedical Department, Francisc I. Rainer Anthropology
Institute of the Romanian Academy, Academy House, Romania
corneliarada@yahoo.com
Abstract. The objectives of this study were the determination of the prevalence of self-reported depressive symptoms by the Geriatric Depression Scale and the influences of variable income, physical activity, socialization and sexual activity. A total of 601 patients aged 55–93 years with a mean age of 67.32 years and a median age of 67 years participated in this study between 2016 and 2017. Non-cooperative people and individuals with strong auditory or visual sensory deficits, severe cognitive deficits, or disorders accompanied by psychotic elements with serious somatic pathology were excluded from the interviews. Employing the SPSS GENLIN procedure, an ordinal logistic model was used. Over ½ of the respondents are within the categories of moderate and severe depression, almost half of the respondents feel that their family incomes are not enough or make it hard to meet their needs, approximately 10% think they are sedentary, over ½ participate in no sexual activity, and over ¼ do not frequently respond with pleasure to partner-initiated sexual relationships. Those who were in the higher depression category perceived their income to be extremely low (p = .001), perceived themselves as sedentary (p < .001), infrequently met with friends or neighbours in their leisure time (p = .002), and had lower sexual interest (p < .001). Middle-aged adults and older adults should learn about the health benefits of physical activity, socialization and sexual activity. Social policies must take into account this low-income segment. Poverty itself can be a contributor to depressive states, and additionally, due to their low incomes, elderly people are at risk of benefiting less from pharmacotherapy and psychotherapy.
Keywords: depression, elderly, income, socialization, sexual behaviour.
Veiksniai, susiję su vidutinio ir vyresnio amžiaus asmenų depresija Rumunijoje
Santrauka. Šio tyrimo tikslas – nustatyti savistata grįstų depresijos simptomų paplitimą Rumunijos vidutinio ir vyresnio amžiaus asmenų imtyje ir įvertinti pajamų, fizinio aktyvumo, bendravimo ir seksualinio aktyvumo kintamųjų prognostinę vertę. 2016–2017 metais tyrime dalyvavo 601 pacientas (55–93 metų, amžiaus vidurkis – 67,32 metų, mediana – 67). Nelinkę bendradarbiauti, pasižymintys stipriais girdimojo arba regimojo suvokimo, pažintiniais sutrikimais, turintys psichozinių simptomų ar pasižymintys rimtomis somatinėmis patologijomis asmenys nedalyvavo tyrime. Analizuojant duomenis, atlikta ranginė logistinė analizė, naudojant SPSS GENLIN procedūrą. Daugiau nei pusė respondentų priskirtini vidutinio sunkumo ir sunkios depresijos lygiui, beveik pusė respondentų jautė, kad jų pajamos nepakankamos arba jiems sunku patenkinti savo poreikius, apie 10 % manė, kad jų gyvenimas yra sėslaus būdo, daugiau kaip pusė respondentų neturėjo jokių seksualinių santykių, daugiau kaip ketvirtadalis neatsakė į partnerio inicijuojamus seksualinius santykius. Tie, kurie pateko į didesnės depresijos kategoriją, suvokė savo pajamas kaip ypač mažas (p = 0,001), suvokė save kaip gyvenančius sėslaus būdo gyvenimą (p < 0,001), laisvalaikiu retai susitiko su draugais ar kaimynais (p = 0,002), mažai domėjosi seksualiniais santykiais (p < 0,001). Remiantis tyrimo rezultatais, vidutinio amžiaus ir vyresnius asmenis reikėtų šviesti apie fizinio aktyvumo, bendravimo ir seksualinio aktyvumo naudą. Vykdant socialinę politiką turėtų būti atsižvelgta į asmenis, gaunančius mažas pajamas. Skurdas gali prisidėti prie depresyvios būsenos, taip pat vyresni žmonės dėl savo mažų pajamų rizikuoja gauti mažesnę farmakoterapinę ir psichoterapinę pagalbą.
Raktažodžiai: depresija, pagyvenę žmonės, pajamos, socializacija, seksualinis elgesys.
Received: 18/11/2019. Accepted: 6/5/2020
Copyright © 2020 Cornelia Rada. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution Licence (CC BY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Depression in elderly people poses the risk of not being diagnosed because it can be confused with other issues; for example, depression might be confused with the side effects of some drugs that mimic depression or individuals just being a sad mood as a result of their partner’s death or because of some painful health issues (Harvard Health Publishing, 2008).
Additionally, elderly people are hesitant to ask for help from a psychologist or from psychiatrist because they think depression is a specific part of advanced age or because they often have a chronic illness that they treat with a doctor in another specialty for financial reasons (Mitchel, 2011).
Age itself is not considered a risk factor for depression in elderly people. A risk factor for depression, which occurs with age, is the loss of a beloved person, especially a partner (Hashim, Eng, Tohit, & Wahab, 2013).
Other risk factors for depression in elderly people are disability and chronic somatic diseases (Verhaak, Dekker, de Waal, van Marwijk, & van Comijs, 2014).
Social factors involved in depression in elderly people can include a change in role, loss of social status, lower income, financial issues (Fernández-Niño, Bonilla-Tinoco, Manrique-Espinoza, Romero-Martínez, & Sosa- Ortiz, 2018), lack of social support (Harandi, Taghinasab, & Nayeri, 2017), and loneliness (Singh & Misra, 2009).
Almost everything regarding mental and physical health is related to socioeconomic status. Socioeconomic status, a multifaceted construct defined by the dimensions of education, occupational position and household net income, can be both a risk factor for some diseases and a factor that can maintain them. The situation of elderly people in retirement, after withdrawal from work activity, indicates a decrease in income as well as a decrease in occupational position, which can be a trigger for depression and anxiety.
Data from 12,484 participants in the Gutenberg Health study, a population-based, prospective, observational single-centre study in western mid-Germany with an age range of 35 to 74 years, stated that household net income predicted the occurrence of elevated depressive symptoms (Schlax et al., 2019).
The data from the WHO Study on Global Ageing and Adult Health (SAGE) conducted from 2007 to 2010 in China, Ghana, India, Mexico, Russian Federation and South Africa, low- and middle-income countries, showed that lower income levels enhanced the chance of depression among older adults (Anand, 2015).
In Romania, important steps have been taken regarding the social assistance of elderly people. The most recent law on this subject, Law 292/2011, starts with the following statement: “Elderly people represent a vulnerable population category with particular needs, due to the physiological limitations and fragility characteristic of the ageing phenomenon”. Based on standard criteria, a team of evaluators, usually mobile, goes to an elder person’s domicile to establish the degree of dependency. In completing the social insurance benefits to cover the risks of old age and health, elderly people benefit from social assistance measures. The socioeconomic, medical and physiological situation is evaluated. Maintenance in one’s own living environment is essential; for this reason, counselling and support are attempted to be offered at home (Parlamentul României, 2011).
However, in Romania, as a result of the decrease in incomes, elderly people are sometimes forced to give up medical services as well as psychotherapy. The settlement process with health insurance companies regarding psychotherapy is difficult. The money for psychotherapy intervention reaches a psychologist through a specialist doctor with whom the psychologist has signed a contract, and for this reason, specialist doctors and psychologists often avoid ending contracts with health insurance companies.
In Romania, the average monthly pension was 1172 RON (Institutul Național de Statistică, 2019) (at the rate as of December 24, 2019, the National Bank of Romania makes 245 euros).
For a clearer picture, it should be noted that in 2017, in the member countries of the European Union, the lowest level of income for elderly people (ranked by the median equivalent of net income of the total population, both sexes, starting at 65 years of age) was registered in Lithuania, Latvia, Bulgaria and Romania (Eurostat Ageing Europe, 2017).
In this study, a subjective indicator of income is used, namely, the perception of income in relation to needs.
Insufficient physical activity is the fourth leading risk factor for mortality (World Health Organization, 2009). “Physical activity includes leisure time physical activity (for example, walking, dancing, gardening, hiking, and swimming), transportation (e.g., walking and cycling), occupational (i.e., work), household chores, play, games, sports and planned exercise in the context of daily, family, and community activities” (World Health Organization, 2017a).
A correlation between low levels of physical activity and symptoms of anxiety and depression in elderly people was found (de Oliveira, Souza, Rodrigues, Fett, & Piva, 2019).
In a sample of 497 Romanian subjects randomly selected during 2011–2012 that were 35–74 years of age, Rada found that with advancing age, the proportion of people who spend their free time watching TV programmes tends to increase, the proportion of those who spend their free time walking outdoors tends to decrease, and the share of those who practice a sport tends to diminish by half (Rada, 2017b).
Here, the perception of the subjects regarding their sedentary behaviour is analysed.
Studies have shown an association between loneliness and multiple diseases (hypertension, heart disease and stroke) for elderly people, and it has been found that loneliness is involved in depressive symptoms, cognitive problems and the development of dementia (Cacioppo, Capitanio, & Cacioppo, 2014).
Here, the social dimension of loneliness as well as the emotional dimension is to be emphasized. For example, in one of the most commonly used scales in Europe, the Loneliness Scale of Jong-Gierveld includes items that evaluate the emotional dimension such as “I experience a general sense of emptiness” and items that evaluate the social dimension such as “There are enough people I feel close to” (de Jong-Gierveld & Kamphuis, 1985).
The Geriatric Depression Scale, which is used in this study, has three explicit items that relate to loneliness: ‘Do you feel that your life is empty? Do you prefer to stay at home, rather than going out and doing new things? Do you prefer to avoid social gatherings?’ (Yesavage et al., 1982).
In a meta-analysis, Ong, Uchino, & Wethington concluded that loneliness research is useful in clarifying the brain mechanisms involved in the association between loneliness, cognitive decline, and depression (Ong et al., 2016).
This study uses the level of socialization measured by the habit of meeting friends and neighbours.
The sexual behaviour of elderly people is poorly studied due to several reasons, such as the assumption that elderly people are considered non-sexually active; the mentality according to which sexual activity is for young people and talking about sex in the case of older people is embarrassing; and the assumption that the sexual activity is strictly related to penetration without considering other forms. These are preconceptions or just myths (Fileborn et al., 2015). Bălăceanu Stolnici & Rada identified in a study of 1,800 respondents aged between 15 and 90 that young respondents assumed that their sexual life would end at approximately 45–55 years old. Many adults and older people in good health believed that one’s sexual life never ends (Bălăceanu Stolnici & Rada, 2007).
It is true that after 60 years of age, the frequency and duration of sexual intercourse and the sexual appetite decrease (Rada & Tarcea, 2010). Additionally, elderly people with chronic diseases face difficulties with regard to sexual activity (Merghati-Khoei, Pirak, Yazdkhasti, & Rezasoltani, 2016). However, sexual activity does not depend upon age, and we should consider the biological and neuroendocrine aspects, general health status, marital and socioeconomic status, environment (rural/urban), and patterns induced by society and family. Sexual activity can also be affected by the death of one’s husband/wife and by physical changes (Lindau et al., 2007).
The importance of sexuality for the human body is the same as in the case of other physiological functions, often hiding problems with other systems in the body. Sexual and vasomotor functions, as well as postmenopausal symptoms, interpenetrate, which is why some vasomotor conditions and postmenopausal symptoms can be successfully treated through regular sexual activity (Radu, 2015).
Erectile dysfunction can predict coronary heart disease. Obesity, sedentarism, hypertension, tobacco use, dyslipidaemia, and diabetes are common risk factors for both conditions. Atherosclerosis of the iliac arteries leads to decreased blood flow to the genitals and consequently to erectile dysfunction. The beta-blockers and statins used to treat heart disease can aggravate erectile dysfunction but can be counteracted with 5-phosphodiesterase-inhibiting drugs that have vasodilatory effects and coronary steal effects and alter fat metabolism, as evidenced by the modification of cholesterol values (Stanca, 2014).
Studies have shown that sexual satisfaction is a good predictor of global life satisfaction in older adults (Skałacka & Gerymski, 2019), which is why this study is concerned with sexual activity.
Depression treatment costs are high, and in elderly people, the association with various physical health issues requires increased attention with regard to prevention. Additionally, there are few studies dedicated to depression in elderly people in the specialized literature, especially those in Romania. These are only two of the reasons why this work is useful. The objectives of this study are to identify the prevalence of self-reported depressive symptoms, the way income is perceived, the self-reported level of physical activity, the prevalence of meeting with friends or neighbours and of sexual pleasure and the correlation between depression and these variables.
Methodology
Participants. A total of 601 patients from the Institute of Ana Aslan National Institute of Gerontology and Geriatrics agreed to participate in the Quantitative and Qualitative Study on Successful Aging, A Psycho-socio-medical Approach on the Third Age that took place between 2016 and 2017. The age of the participants was between 55–93 years with a mean of 67.32 and a median of 67. Non-cooperative people and individuals with strong auditory or visual sensory deficits, severe cognitive deficits, or disorders accompanied by psychotic elements with serious somatic pathology were excluded from the interviews.
Tasks and Methods of Evaluation. Several questionnaires were administered, including personality, memory, quality of life, and depression questionnaires and an omnibus-type questionnaire, with 36 items that collected sociodemographic data, data on behaviours harmful for health, and opinions and attitudes relevant to the health of elderly people. The questionnaires were completed in the form of face-to-face interviews with each patient. These interviews were conducted by specialists in clinical psychology and psychotherapists, with experience in geriatrics, gerontology and working with elderly people. The response rate was 100%.
Informed written consent was obtained from each participant at the time of recruitment. The subjects were informed that they could withdraw from the study at any stage, and confidentiality was assured. The study was approved by the Ethics Commission, No. 153/1 March 2016. Ethics approval and consent to participate are available upon request.
For this article, the Geriatric Depression Scale long form and 4 items from the omnibus type questionnaire are used. This study is a part of the larger research, more about the methodology, the sample structure, and instruments can be found in other articles that have used data collected in the abovementioned research (Rada, 2017a).
Instruments and Statistical Analyses. The Geriatric Depression Scale long form (GDS) was used, a questionnaire in which participants are asked to respond by answering yes or no in reference to how they felt over the past week. The 30 items specifically target common depression symptoms in older adults. This questionnaire mainly measures psychological and psychiatric symptoms rather than somatic symptoms (Budson & Solomon, 2016).
The original scoring for the scale is one point for each of these answers. Cutoff: normal-0-9; mild depression-10-19; severe depression-20-30. The scale has good validity and reliability (Yesavage et al., 1982). The scale can be used free of charge, translated into several languages and validated in many cultural spaces. The adaptation and validation of the GDS was made for the Romanian population and indicated good psychometric properties (Ștefan & Băban, 2017).
The next four items were also used: I. How do you estimate your total family income considering your necessities? Variants of response: 1. Not enough for our basic needs (food, bills, medicines), 2. Good enough for only our basic needs, 3. Enough for our basic needs, but we cannot afford to purchase more expensive objects (furniture, luxurious clothes, a car, a house), 4. We manage to purchase some expensive objects with some effort, 5. We manage to obtain all desired items without much effort. II. Taking into account the types of activities you do over a week, how would you describe yourself? Variants of response: 1. A sedentary person, 2. An active person, 3. An extremely active person. III. To what extent do you spend time meeting friends and neighbours? Leisure time is defined as the time available after you return from your place of work and on weekends, after shopping, after you have finished your housework, and at the conclusion of all daily chores. Vacation is not counted as leisure time. Variants of response: 1. A little, almost not at all, 2. A lot. IV. How often are you happy to participate in sexual activity initiated by your partner? Variants of response: 1. Very often, 2. Often, 3. Rarely, 4. Very Rarely, 5. No sexual life.
Employing the SPSS GENLIN procedure, an ordinal logistic model was used to predict the geriatric depression category (1 = Normal, 2 = Mild, 3 = Severe) on four other categorical variables describing income satisfaction perception (1 = Extremely Low, 2 = Low, 3 = Decent, 4 = Satisfactory, 5 = Very Satisfactory), physical activity self-perception (1 = Sedentary, 2 = Active, 3 = Very Active), frequency of leisure time habit to meet people (1 = Rarely, 2 = Often) and frequency of sexual interest (1 = Very Often, 2 = Often, 3 = Rarely, 4 = Very Rarely, 5 = No sexual life).
The deviance and Pearson goodness-of-fit tests indicated that the model was a good fit to the observed data, χ2 (167) = 150.607, p = .902 for deviance and χ2 (167) = 148.207, p = .887 for Pearson. Both the omnibus test and tests of model effects were significantly lower than p < .05 and indicated that the current model outperforms the null model (intercept only), and each of the main-effects terms of the four predictors contributed to the model.
The hypotheses of this study are as follows: the risk of depression is lower if there are a) a perception of income as satisfactory in terms of needs; b) a perception of one’s own person as being active; c) socialization with neighbours and friends; and d) sexual activity with pleasure.
Results
Table 1 displays the basic structure of the sample important for this study.
Table 1. Relevant Sociodemographic Characteristics of the Participants
|
Sociodemographic data |
N |
% |
|
Gender |
||
|
Female |
492 |
81.9 |
|
Male |
109 |
18.1 |
|
Age groups (years) |
||
|
55–64 |
224 |
37.3 |
|
65–74 |
272 |
45.3 |
|
75–79 |
70 |
11.6 |
|
80+ |
35 |
5.8 |
|
Marital status |
||
|
Married |
318 |
52.9 |
|
Widowed |
202 |
33.6 |
|
Divorced |
55 |
9.2 |
|
Consensual union over 1 year |
19 |
3.2 |
|
Unmarried (single) |
7 |
1.2 |
|
Personal monthly income* |
|
|
|
Less or equal to 215 EUR |
224 |
37.3 |
|
216–429 |
289 |
48.1 |
|
430–644 |
57 |
9.5 |
|
645–858 |
13 |
2.2 |
|
Over 858 EUR |
18 |
3.0 |
*Conversion of RON into EUR, according to the National Bank of Romania exchange rate on April 5, 2018.
All the subjects answered the questionnaires. Therefore, all the results refer to the entire sample N = 601.
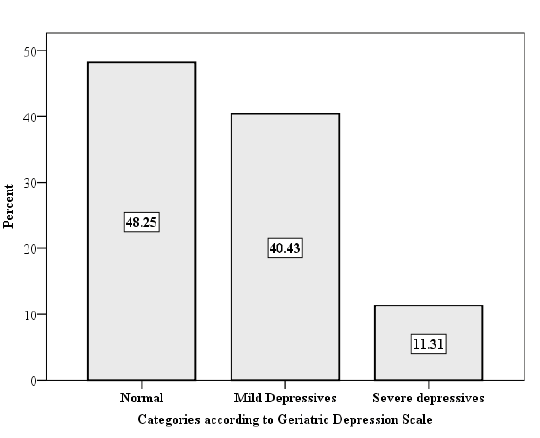
Figure 1. Distribution of Respondents According to Geriatric Depression Scale
Figure 1 shows that over ½ of respondents are in the moderate and severe depression categories at the time of the interview.
Figure 2 shows that 47.25% of the respondents consider their family income to not be enough to cover or to hardly cover basic needs.
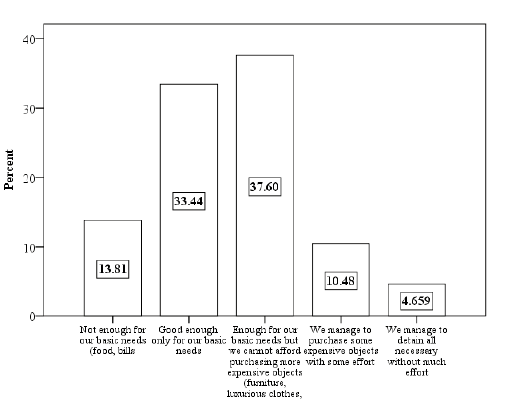
Figure 2. Respondent Distribution According to the Perception of Family Income
Figure 3 shows that almost 90% of the respondents consider themselves to be active or very active people.
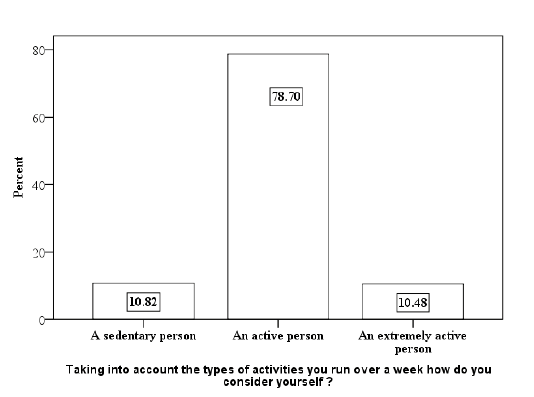
Figure 3. Respondent Distribution According to Self-Perception Taking into Account Activities within a Week
Figure 4 shows that over ½ of the respondents do not have sexual life (regardless of marital status) and over ¼ do not respond with pleasure to the sexual activities initiated by their partners.
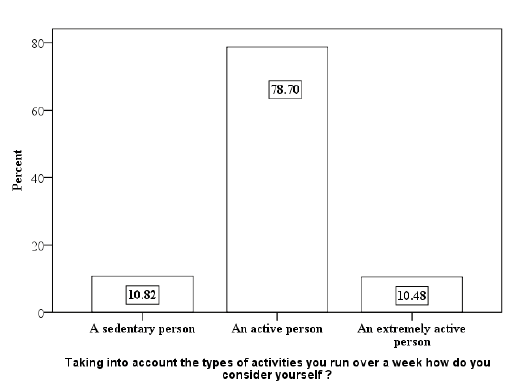
Figure 4. Respondent Distribution According to Pleasure with Sexual Activity
Figure 5 shows that almost ¾ of the respondents do not frequently spend their leisure time meeting with friends or neighbours.
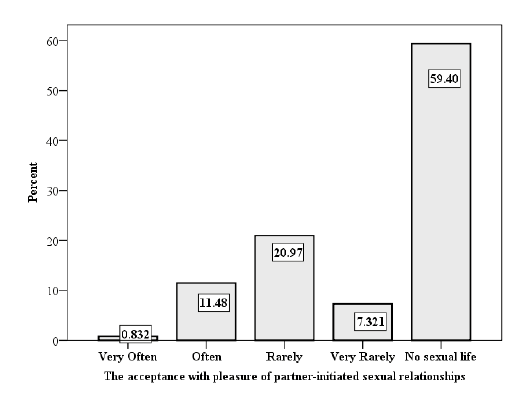
Figure 5. Respondent Distribution According to Meeting with Friends and Neighbours
The employed model indicate that for people who consider their income to be extremely low, the odds of scoring higher (being in a higher depression category) on the dependent variable (high depression category) are nearly 5.1 higher than those for the people with very satisfactory income. The odds ratio of being in a higher category of the dependent variable for the depression category is 5.077 (95% CI, 2.017 to 12.782), a statistically significant effect, χ2 (1) =11.898, p = .001.
The odds of being in a higher category for the dependent variable (high depression category) is significantly higher for the people who perceived themselves as sedentary than for people who declared themselves to be very active. The odds ratio of being in a higher category of the dependent variable of depression category is 3.935 (95% CI, 1.909 to 8.113), a statistically significant effect, χ2 (1) = 13.773, p < .001.
Sexual interest is also significant for depression category prediction. The odds ratio of being in a higher category of the dependent variable of depression is lower (< 1) when the respondent has sexual interests than when the respondent has no sexual life. The model indicates that the odds ratio of being in a higher category of the dependent variable of depression for people with sexual interests is 0.326 lower (95% CI, 0.181 to .588) than that of people without sexual desire. The effect is statistically significant, χ2 (1) = 13.893, p < .001 for the people who are often interested in sexual provocations. This also means that the odds ratio of being in a higher category of depression is 1/0.326 = 3.06 higher for people with no sexual life than for people often interested in sexual provocations.
Regarding the habit of meeting people as a leisure time activity, the model indicates that the odds of being in a higher category for the dependent variable (high depression category) is significantly higher than those for people who have meetings with some other people (friends, neighbours, etc.). The odds ratio of being in a higher category of the dependent variable for depression category is 1.795 (95% CI, 1.248 to 2.582), a statistically significant effect, χ2 (1) = 9.962, p = .002 (Table 2).
Table 2. Parameter Estimates
|
Parameter |
B |
Std. Error |
95% Wald |
Hypothesis Test |
Exp(B) |
95% Wald |
|||||
|
Lower |
Upper |
Wald |
df |
Sig. |
Lower |
Upper |
|||||
|
Threshold |
[GDScateg = 1] |
1.576 |
.5071 |
.582 |
2.570 |
9.662 |
1 |
.002 |
4.837 |
1.790 |
13.067 |
|
[GDScateg = 2] |
3.964 |
.5300 |
2.926 |
5.003 |
55.949 |
1 |
.000 |
52.694 |
18.647 |
148.905 |
|
|
I. Perception of family income |
1 |
1.625 |
.4711 |
.702 |
2.548 |
11.898 |
1 |
.001 |
5.077 |
2.017 |
12.782 |
|
2 |
1.305 |
.4417 |
.439 |
2.171 |
8.732 |
1 |
.003 |
3.688 |
1.552 |
8.766 |
|
|
3 |
.557 |
.4404 |
–.306 |
1.420 |
1.601 |
1 |
.206 |
1.746 |
.736 |
4.139 |
|
|
4 |
.093 |
.5019 |
–.891 |
1.077 |
.034 |
1 |
.853 |
1.098 |
.410 |
2.936 |
|
|
5 |
0a |
. |
. |
. |
. |
. |
. |
1 |
. |
. |
|
|
II. Physical activity |
1 |
1.370 |
.3691 |
.646 |
2.094 |
13.773 |
1 |
.000 |
3.935 |
1.909 |
8.113 |
|
2 |
.570 |
.2920 |
–.002 |
1.143 |
3.817 |
1 |
.051 |
1.769 |
.998 |
3.135 |
|
|
3 |
0a |
. |
. |
. |
. |
. |
. |
1 |
. |
. |
|
|
II. Interest in sexual activity |
1 |
–.850 |
.9561 |
–2.723 |
1.024 |
.790 |
1 |
.374 |
.428 |
.066 |
2.785 |
|
2 |
–1.121 |
.3007 |
–1.710 |
–.532 |
13.893 |
1 |
.000 |
.326 |
.181 |
.588 |
|
|
3 |
–.150 |
.2057 |
–.553 |
.253 |
.533 |
1 |
.465 |
.861 |
.575 |
1.288 |
|
|
4 |
–.930 |
.3392 |
–1.594 |
–.265 |
7.510 |
1 |
.006 |
.395 |
.203 |
.767 |
|
|
5 |
0a |
. |
. |
. |
. |
. |
. |
1 |
. |
. |
|
|
IV. Socialization |
1 |
.585 |
.1854 |
.222 |
.948 |
9.962 |
1 |
.002 |
1.795 |
1.248 |
2.582 |
|
2 |
0a |
. |
. |
. |
. |
. |
. |
1 |
. |
. |
|
|
(Scale) |
1b |
|
|
|
|
|
|
|
|
|
|
Dependent Variable: Category on Depression Geriatric Scale (Normal, Mild, Severe). Model: (Threshold), I. Perception of family income, II. Self-perception taking into account the activities within a week, III. Interest in sexual activity, IV. Meetings with friends, neighbours. a. Set to zero because this parameter is redundant. b. Fixed to the displayed value.
Discussion
The results of the employed ordinal logistic model should not be necessarily interpreted in terms of a direct influence of independent variables on the depression level variable in a causal relationship. This non-experimental study was based on an administered questionnaire, without any manipulations of independent variables. While it was not possible to identify the cause and effect between the variables, we could still examine the association or relationship between them. However, the assumption of direct influence from the independent variables on the depression level could not be excluded.
Self-Reported Depressive Symptoms by GDS
The prevalence of self-reported depressive symptoms in the current study is over 50%, out of which severe depression is over 11%. This indicates a high prevalence in comparison with other studies. Barua, Ghosh, Kar and Basilio (2011) conducted a retrospective study regarding the prevalence of depressive disorders in the elderly populations in Asia, Europe, Australia, North America, and South America, from 74 studies published in indexed journals between 1955 and 2005 and found a median prevalence rate of depressive disorders of 10.3% (varying between 4.7% and 16.0%) (Barua et al., 2011). The prevalence of self-reported depressive symptoms in the current study is higher than that Mirkena, Reta, Haile, Nassir and Sisay (2018) found in a study of 800 older adults (age ≥ 60 years) in Ambo Town, Ethiopia, in 2016, where the prevalence of depression was 41.8% (Mirkena et al., 2018).
The prevalence of self-reported depressive symptoms in the current study is lower than that Goyal and Kajal (2014) found in a study of 100 elderly people over 60 years old from the Southern Part of Punjab, India, where the prevalence of severe depression was 17% and that of mild depression was 60%. The World Health Organization estimated that approximately 7% of adults aged over 60 all over the world are affected by depression (World Health Organization, 2017b), and in the sample used in the current research, the prevalence of depression is much higher.
self-reported depressive symptoms (Doshi, Cen, & Polsky, 2008).
In Romania, between July 1977 and March 2001, the retirement age limit was 62 years for men and 57 for women (Marea Adunare Nationala, 1977). According to the law issued in 2010, the standard retirement age is 63 years for women and 65 years for men. For women, the extension will be performed gradually by January 2030 (Casa Naţională de Pensii Publice, 2017). may extend their activity. For example, the retirement age for research and development staff is 65 years for both women and men (Parlamentul României, 2018).
Depression – Unsatisfactory Income
The current study reveals that nearly half of the respondents feel that their family income is not enough to meet basic needs or make it hard to meet basic needs. In most cases, a pension is lower than the income earned as an employee. As a result, the impact of diminishing the income of elderly people after retirement is a highly discussed topic.
This result is similar to those of most studies, which have found that among low-income people, the prevalence of depression is higher (Mohd Sidik, Mohd Zulkefli, & Shah, 2003; Sharma et al., 2016).
The current study identifies that the respondents who considered their family income to be too low to cover basic needs (not enough for our basic needs; good enough for only our basic needs) have the highest probability of belonging to a category of depressive people. There may be differences between the perception of income in relation to needs and real income, but there is a correlation between them in this study. Consequently, for 37.3% of the subjects, their personal monthly income is less than or equal to 215 EUR (See Table 1). We can suggest that in the studied sample of elderly individuals, there is also an association between depression and low income.
Depression – Sedentarism – Low Socialization with Friends/Neighbours
In the present study, an association is identified between those who reported being sedentary and depression. This result is in line with that obtained by the team of Stubbs et al. among 42,469 people in low- and middle-income countries, which showed that people with depression, especially elderly people, spend time more sedentarily than those without depression (Stubbs et al., 2018).
There is scientific evidence to support the benefits of physical exercise on health in general and on depressive disorders in particular in older adults (López-Torres Hidalgo, 2019).
Urgent measures are needed to promote behavioural activation in elderly people so that they perform physical activity in all forms (walking, dancing, gardening, hiking, swimming, games, sports, etc.), reducing the burden on mental health costs, which may be an alternative to antidepressant drugs.
The current study shows that almost ¾ of the respondents do not spend their free time meeting with friends and neighbours, which indicates a low level of socialization. This can be a consequence of retirement, when the professional subidentity dissolves and family and sociocultural subidentities become less compact and fade. The habit of not meeting people is associated with depression. This is in agreement with the results of most studies, which reveal that after retirement, elderly people tend to interact and socialize less, which increases the risk of isolation, loneliness, and depression.
Additionally, this result suggests that the relations with family and friendships are important for the well-being of older adults (Nguyen, Chatters, Taylor, & Mouzon, 2016).
Telephone or e-mail contact and especially socialization face to face socialization are anti-depressive factors (Teo et al., 2015). There is a reason why socializing with friends or neighbours should be encouraged.
There may be a vicious circle that needs to be broken. Depression itself is manifested by withdrawal from ordinary activities even through inappropriate socialization, etc. On the other hand, sedentarism and preference for loneliness are risk factors for depression.
In addition, spending time mostly sedentarily leads to and strengthens a number of age-related illnesses such as heart and cardiovascular diseases, diabetes mellitus, and decreases in muscle tone, and generally leads to premature ageing and to a low life expectancy (Rada, 2017b).
Depression – Absent Sexual Life and Reduced Sexual Pleasure
In the present study, almost half of the respondents have a sexual life, and over 12% respond with pleasure often and very often to partner-initiated sexual intercourse. Low enjoyment of sexual intercourse as well as lack of a sexual life is associated with depression, which is consistent with the results other studies (Ganong & Larson, 2011).
This is also a risk for a vicious circle that needs to be broken, because anxiety and depression are risk factors for triggering sexual dysfunction, and in turn, sexual dissatisfaction can lead to a decrease in the appetite for life.
Love and sexual life should not be associated only with youth. Sexual pleasure contributes to high morale and can even prolong life. Sex, sexuality, and intimacy help elderly people feel joy of life and feel lively and strengthens their relationships. It seems inappropriate to talk about sexual education to elderly people; however, psychologists should provide family doctors, urologists, gynaecologists, endocrinologists, cardiologists and doctors of other specialties with a minimal set of sex-related information about the sexual lives of elderly people, such as those described below. Approaching the subject of elderly sexuality without inhibition (but with measure) is a sign of social maturity. Faced with erotic and sexual impulses, elderly people should not feel guilty, and young people should not ridicule them.
Sexual dysfunctions cause some men to use testosterone pills, and after seeing that they do not function as they wish or they take into account the risks of hormone therapy, they withdrawal from sexual activity. Women can also have sex-related pain related to lack of lubrication, which makes them avoid sexual intercourse, although there are treatments for women at menopause. It is normal for men and women to notice a gradual decrease in libido as they age, which is a hormone-related aspect. However, sex includes not only penetration but also erotic context, caresses, erotic massage, enthusiastic attachment, emotional intimacy, stability, continuity and more.
Studies have shown an association between testosterone replacement therapy and myocardial infarction. For this reason, it is necessary to insist on lifestyle changes, performance of daily physical movement and regulation of the periodicity of sexual life, all of which lead to the normalization of endogenous testosteronemia (Stoian, 2014).
With increasing life expectancy, in the 21st century, the medical perspective on sexual activity has joined the social-relational perspective ( 2015).
In conclusion, the assumptions of the study are confirmed: the moderate and severe depression categories of GDS, obtained through self-reported depressive symptoms, are associated with unsatisfactory income, sedentarism, low socialization with neighbours or friends and no sexual activity or sexual activity without pleasure.
Because interventions for the diagnosis and treatment of depression are expensive, exit from the labour market should be taken into account in public health policies regarding possible depression.
Because of their low incomes, elderly people may be less likely to benefit from pharmacotherapy and psychotherapy. Financial insecurity in older age may lead to poverty and other forms of social exclusion in which intervention in depression becomes more complicated. For this reason, increased attention should be paid to the management of low-income elderly people.
A good example in this regard is that proposed by Areán et al., which consists of a combination of programmes aimed at bringing food home for elderly people and teaching older people a problem-solving model in 7 steps (Areán et al., 2010).
Elderly people should receive information about the prevention and treatment of depression. It is also useful to openly and honestly address the subject of sexual activity without exaggerated inhibitions because dynamics and sexual pleasure can be both a trigger factor and a prevention factor of depression.
Psychotherapists have an important role to play in this regard by providing elderly people with techniques to get them motivated to continue living and adapting to the environment and to its challenges, such as cognitive behavioural therapy, scheme therapy, and narrative therapy. Older people should be encouraged to engage in volunteer activities, meet with neighbours and friends, engage in daily physical exercise, and engage in prolonged outdoor walks, and they should be constantly reminded of the benefits of these behaviours.
In general, the problem in Romania is not how psychologists and psychiatrists work in diagnosing and treating depression in elderly people, but it is the fact that they do not arrive or arrive late to psychologists/psychiatrists. Family doctors and specialists in other fields dealing with chronic diseases in elderly people are called to be vigilant in identifying depression symptoms. A simple method could be to use the Geriatric Depression Scale short form 15 items (Sheikh & Yesavage, 1986). It takes approximately 5 to 7 minutes to complete. Depending on the scores, it would be necessary to send the patient to a specialist psychologist and/or psychiatrist. Here, the collaboration of the psychologist with the doctor becomes especially important. Older people often have comorbid conditions and are treated for these; as a result, consideration should be given to the possibility that the affective symptoms may be caused by the physiological effects of the disease (for example, depression after stroke, common in elderly people) but also as a result of drugs (for example, cardiovascular agents, drugs that act upon the central nervous system, antibiotics and chemotherapeutic agents) (American Psychiatric Association, 2016, pp. 175–182).
This study has some limitations, the most important being the following. This article is based on the self-reporting of depressive symptoms based on category of GDS to which the subject belongs, which can be misleading regarding the diagnosis of depression. For this reason, to establish this diagnosis, a deeper evaluation of anamnesis is necessary.
The patients in this study do not have severe pathology and are hospitalized in this institute approximately twice a year for regular treatments, especially for gerovital or aslavital treatments, one of the most powerful Romanian brands, well known in the world for the positive effects in geriatrics. However, we must take into account that the answers to the GDS can be distorted by the hospitalization situation that the respondent is in.
The fact that the sample was small and unbalanced in gender structure, age groups, and residence limits the generalization of the results of this study, as well as the comparisons of these socio-demographic variables. The study did not take into account other risk factors for depression. It should also be noted that the GDS does not replace an in-depth psychological assessment to diagnose depression (American Psychiatric Association, 2016, pp. 155–188), but it can be used to monitor depression and any score indicating depression. It is to be considered for possible intervention and prompt treatment.
However, these results can be a starting point in policies to prevent depression for elderly people approaching retirement and during retirement and to emphasize the importance of income, physical activity, socialization and sexual behaviour. These factors considered in the analysis that may be involved in depression demonstrate the need for interventions on several levels, such as social policies and public health policies through permanent information and prevention campaigns.
References
American Psychiatric Association. (2016). Manual de diagnostic și clasificare statistică a tulburărilor mintale [The diagnostic and statistical manual of mental disorders]. American Psychiatric Association.
Anand, A. (2015). Understanding depression among older adults in six low-middle income countries using WHO-SAGE survey. Behavioral Health, 1 (2), 1–11.
Areán, P. A., Mackin, S., Vargas-Dwyer, E., Raue, P., Sirey, J. A., Kanellopolos, D., & Alexopoulos, G. S. (2010). Treating depression in disabled, low-income elderly: A conceptual model and recommendations for care. International Journal of Geriatric Psychiatry, 25 (8), 765–769. https://doi.org/10.1002/gps.2556
Bălăceanu Stolnici C., & Rada, C. (2007). Coordinates of the sexual behaviour at the third age, International conference in gerontology. In F. Schneider, D. Podea, & P. Nanu (Eds.), The International conference in gerontology (pp. 119–126). Viaţa Medicală Românescă.
Barua, A., Ghosh, M. K., Kar, N., & Basilio, M. A. (2011). Prevalence of depressive disorders in the elderly. Annals of Saudi Medicine, 31 (6), 620–624. https://doi.org/10.4103/0256-4947.87100
Budson, A. E., & Solomon, P. R. (2016). Evaluating the patient with memory loss or dementia in memory loss, Alzheimer’s disease and dementia. Elsevier.
Cacioppo, S., Capitanio, J. P., & Cacioppo, J. T. (2014). Toward a neurology of loneliness. Psychological Bulletin, 140 (6), 1464–1504. https://doi.org/10.1037/a0037618
Casa Naţională de Pensii Publice. (2010). Legea nr. 263/2010 privind sistemul de pensii publice, Pensia pentru limita de varsta. [National House of Public Pensions 2010. Law no. 263/2010 on the unitary pension system, Pension for old age]. https://www.cnpp.ro/pensia-pentru-limita-de-varsta
de Jong-Gierveld, J., & Kamphuls, F. (1985). The development of a rasch-type loneliness scale. Applied Psychological Measurement, 9 (3), 289–299. https://doi.org/10.1177/014662168500900307
de Oliveira, L. D. S. S. C. B., Souza, E. C., Rodrigues, R. A. S., Fett, C. A., & Piva, A. B. (2019). The effects of physical activity on anxiety, depression, and quality of life in elderly people living in the community. Trends in Psychiatry and Psychotherapy, 41 (1), 36–42. https://doi.org/10.1590/2237-6089-2017-0129
DeLamater, J., & Koepsel, E. (2014). Relationships and sexual expression in later life: A biopsychosocial perspective. Sexual and Relationship Therapy, 30 (1), 37–59. https://doi.org/10.1080/14681994.2014.939506
Doshi, J. A., Cen, L., & Polsky, D. (2008). Depression and retirement in late middle-aged U.S. workers. Health Services Research, 43 (2), 693–713. https://doi.org/10.1111/j.1475-6773.2007.00782.x
Eurostat Ageing Europe. (2017). Statistics on pensions, income and expenditure. https://ec.europa.eu/eurostat/statistics-explained/index.php?title=File:Median_equivalised_net_income,_by_sex_and_age_class,_2017_(PPS)_AE2019.png
{kind=link}
Fernández-Niño, J. A., Bonilla-Tinoco, L. J., Manrique-Espinoza, B. S., Romero-Martínez, M., & Sosa-Ortiz, A. L. (2018). Work status, retirement, and depression in older adults: An analysis of six countries based on the study on global ageing and adult health (SAGE). SSM-Population Health, 6, 1–8. https://doi.org/10.1016/j.ssmph.2018.07.008
Fileborn, B., Thorpe, R., Hawkes, G., Minichiello, V., Pitts, M., & Dune, T. (2015). Sex, desire and pleasure: Considering the experiences of older Australian women. Sexual and Relationship Therapy, 30 (1), 117–130. https://doi.org/10.1080/14681994.2014.936722
Ganong, K., & Larson, E. (2011). Intimacy and belonging: The association between sexual activity and depression, among older adults. Society and Mental Health, 1 (3), 153–172. https://doi.org/10.1177/2156869311431612
Goyal, A., & Kajal, K. S. (2014). Prevalence of depression in elderly population in the southern part of Punjab. Journal of Family Medicine and Primary Care, 3 (4), 359–361. https://doi.org/10.4103/2249-4863.148109
Harandi, T. F., Taghinasab, M. M., & Nayeri, T. D. (2017). The correlation of social support with mental health: A meta-analysis. Electronic Physician, 9 (9), 5212–5222. https://doi.org/10.19082/5212
Harvard Health Publishing. (2008). Recognizing and treating depression in the elderly. https://www.health.harvard.edu/newsletter_article/Recognizing_and_treating_depression_in_the_elderly
Hashim, S. M., Eng, T. C., Tohit, N., & Wahab, S. (2013). Bereavement in the elderly: The role of primary care. Mental Health in Family Medicine, 10 (3), 159–162.
Institutul Național de Statistică. (2019). Comunicat de presă, Nr.74 /29.03.2019 [Press Release, No.74 / 29.03.2019]. http://www.insse.ro/cms/sites/default/files/com_presa/com_pdf/pensii_2018r.pdf
Lindau, S. T., Schumm, L. P., Laumann, E. O., Levinson, W., O’Muircheartaigh, C. A., & Waite, L. J. (2007). A study of sexuality and health among older adults in the United States. New England Journal of Medicine, 357 (8), 762–774. https://doi.org/10.1056/nejmoa067423
López-Torres Hidalgo, J. (2019). Effectiveness of physical exercise in the treatment of depression in older adults as an alternative to antidepressant drugs in primary care. BMC Psychiatry, 19 (1), 21. https://doi.org/10.1186/s12888-018-1982-6
Marea Adunare Nationala. (1977). Legea nr 3 din 30/6 /77 privind pensiile de asigurari sociale de stat si asistenta sociala, Aparuta in Buletinul Oficial nr. 82 din 6 /8 /77. [Grand National Assembly 1977. law no 3 of 30/6 / 77 on state social insurance and social assistance pensions, published in the Official Bulletin no. 82 of 6/8/77]. http://www.cdep.ro/pls/legis/legis_pck.htp_act_text?idt=1356
Merghati-Khoei, E., Pirak, A., Yazdkhasti, M., & Rezasoltani, P. (2016). Sexuality and elderly with chronic diseases: A review of the existing literature. Journal of Research in Medical Sciences, 21 (1), 136. https://doi.org/10.4103/1735-1995.196618
Mirkena, Y., Reta, M. M., Haile, K., Nassir, Z., & Sisay, M. M. (2018). Prevalence of depression and associated factors among older adults at ambo town, Oromia region, Ethiopia. BMC Psychiatry, 18 (1), 338. https://doi.org/10.4103/1735-1995.196618
Mitchell, A. J. (2011). Why do physicians have difficulty diagnosing depression in the elderly? Aging Health, 7 (1), 99–101. https://doi.org/10.2217/ahe.10.67
Mohd Sidik, S., Mohd Zulkefli, N. A., & Shah, S. A. (2003). Factors associated with depression among elderly patients in a primary health care clinic in Malaysia. Asia Pacific Family Medicine, 2 (3), 148–152. https://doi.org/10.1046/j.1444-1683.2003.00080.x
Nguyen, A. W., Chatters, L. M., Taylor, R. J., & Mouzon, D. M. (2016). Social support from family and friends and subjective well-being of older African Americans. Journal of Happiness Studies, 17 (3), 959–979. https://doi.org/10.1007/s10902-015-9626-8
Ong, A. D., Uchino, B. N., & Wethington, E. (2016). Loneliness and health in older adults: A mini-review and synthesis. Gerontology, 62(4), 443–449. https://doi.org/10.1159/000441651
Parlamentul României. (2011). Legea asistenţei sociale Nr. 292/2011, Publicată în Monitorul Oficial nr. 905/20 dec. 2011 [The Law of social assistance Nr. 292/2011, published in the Official Gazette no. 905/20 dec. 2011]. http://www.mmuncii.ro/pub/imagemanager/images/file/Legislatie/LEGI/L292-2011.pdf
Parlamentul României. (2018). Legea nr. 69 din 19 martie 2018 pentru completarea Legii nr. 319/2003 privind Statutul personalului de cercetare-dezvoltare, articol 35^1, Monitorul Oficial. (2018). Nr. 245 din 20 martie 2018, [The Law no. 69 of March 19, 2018 for the completion of Law no. 319/2003 regarding the Statute of the research and development staff, article 35^1, the Official Monitor, no. 245 of March 20, 2018].
Rada, C. (2017a). Latent class analysis approach for the family adaptability and cohesion evaluation scale IV among young people from Romania: The first step for validation. Journal of Family Issues, 39 (6), 1598–1615. https://doi.org/10.1177/0192513x17714508
Rada, C. (2017b). Impact of some demographic parameters on leisure time and body weight. Anthropological Researches and Studies, 7 (1), 111–121. https://doi.org/10.26758/7.1.12
Rada, C., & Tarcea, M. (2010). Viaţa sexuală şi familia în mediul urban românesc. Studiul Rada-Tarcea [Sexual and family life of the Romanians. Study Rada–Tarcea]. Institutul European.
Radu, O. (2015). Sexualitatea–indicator pentru sănătate [Sexuality-health indicator]. http://www.amsr.ro/pdf/articol-amsr-xv-sexualitatea.pdf
Schlax, J., Jünger, C., Beutel, M. E., Münzel, T., Pfeiffer, N., Wild, P., Blettner, M., Kerahrodi, J. G., Wiltink, J., & Michal, M. (2019). Income and education predict elevated depressive symptoms in the general population: Results from the Gutenberg health study. BMC Public Health, 19 (1), 430. https://doi.org/10.1186/s12889-019-6730-4
Sharma, K., Gupta, A., Sharma, R., Mahajan, N., Mahajan, A., Sharma, D., & Mazta, S. (2016). Prevalence and risk factors for depression in elderly North Indians. Journal of Geriatric Mental Health, 3 (2), 158–163. https://doi.org/10.4103/2348-9995.195673
Sheikh, J. I., & Yesavage, J. A. (1986). Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clinical Gerontologist: The Journal of Aging and Mental Health, 5 (1–2), 165–173. https://doi.org/10.1300/J018v05n01_09
Singh, A., & Misra, N. (2009). Loneliness, depression and sociability in old age. Industrial Psychiatry Journal, 18 (1), 51–55. https://doi.org/10.4103/0972-6748.57861
Skałacka, K., & Gerymski, R. (2019). Sexual activity and life satisfaction in older adults. Psychogeriatrics, 19 (3), 195–201. https://doi.org/10.1111/psyg.12381
Stanca, I. (2014). Corelații ale disfuncției erectile cu boala cardiacă ischemică [Correlations of erectile dysfunction with ischemic heart disease]. Buletinul Oficial al A.M.S.R. Info Medicina Sexualității, 1, 14.
Ștefan, A. M., & Băban, A. (2017). The Romanian version of the geriatric depression scale: Reliability and validity. Cognition, Brain, Behavior. An Interdisciplinary Journal, 21 (3), 175–187. https://doi.org/10.24193/cbb.2017.21.10
Stoian, D. (2014). Controversele terapiei de substituție cu testosterone la bărbatul adult [Controversies of testosterone replacement therapy in adult men]. Buletinul Oficial al A.M.S.R. Info Medicina Sexualității, 1, 15.
Stubbs, B., Vancampfort, D., Firth, J., Schuch, F. B., Hallgren, M., Smith, L., Gardner, B., Kahl, K. G., Veronese, N., Solmi, M., Carvalho, A. F., & Koyanagi, A. (2018). Relationship between sedentary behavior and depression: A mediation analysis of influential factors across the lifespan among 42,469 people in low- and middle-income countries. Journal of Affective Disorders, 229, 231–238. https://doi.org/10.1016/j.jad.2017.12.104
Teo, A. R., Choi, H., Andrea, S. B., Valenstein, M., Newsom, J. T., Dobscha, S. K., & Zivin, K. (2015). Does mode of contact with different types of social relationships predict depression in older adults? Evidence from a nationally representative survey. Journal of the American Geriatrics Society, 63 (10), 2014–2022. https://doi.org/10.1111/jgs.13667
Verhaak, P. F. M., Dekker, J. H., de Waal, M. W. M., van Marwijk, H. W. J., & van Comijs, H. C. (2014). Depression, disability and somatic diseases among elderly. Journal of Affective Disorders, 167, 187–191. https://doi.org/10.1016/j.jad.2014.05.057
World Health Organization. (2009). Global health risks: Mortality and burden of disease attributable to selected major risks. World Health Organization Press.
World Health Organization. (2017a). Global strategy on diet, physical activity and health, physical activity and adults. World Health Organization.
World Health Organization. (2017b). Mental health of older adults. World Health Organization.
Yesavage, J. A., Brink, T. L., Rose, T. L., Lum, O., Huang, V., Adey, M., & Leirer, V. O. (1982). Development and validation of a geriatric depression screening scale: A preliminary report. Journal of Psychiatric Research, 17 (1), 37–49. https://doi.org/10.1016/0022-3956(82)90033-4