Socialiniai tyrimai eISSN 2351-6712
2022, vol. 45(1), pp. 36–47 DOI: https://doi.org/10.15388/Soctyr.45.1.2
Exploring the Relationship between Self-Control and Healthy Eating: Do Self-Description as a Healthy Eater and Attached Importance to Healthy Eating Matter?
Justina Paluckaitė
Utrechto universitetas, psichologijos magistrė
Utrecht University, MSc in psychology
El. p.: justinapaluckaite@gmail.com
Summary. As suggested by previous research, individuals with high self-control report greater autonomous motivation, and the Self-Determination Theory of autonomous motivation implies that exercising self-control should be less necessary, i.e., require lower levels for those having a self-schema in the relevant domain. Based on this, the present study explored whether the healthy eater self-schema status decreases (moderates) the effect of the trait self-control on the healthy eating behavior. In a cross-sectional design, a total of 149 people participated in this research. Results confirmed the role of the healthy eater self-schema status as a moderator. These findings highlighted the effect of the self-description as a healthy eater and one’s perceived importance of healthy eating in the exercising of trait self-control towards healthy food consumption. This study could also be helpful in tailoring future self-control interventions for individuals who have difficulties in exercising self-control toward healthy food consumption.
Keywords: healthy eater self-schema status, trait self-control, healthy eating behavior, young people.
Savikontrolės ir sveikos mitybos ryšys: kokia yra savęs laikymo sveikai besimaitinančiu ir dėmesio skyrimo sveikam maistui rolė?
Santrauka. Praeityje atlikti tyrimai liudija, kad asmenys, turintys aukštą savikontrolę, pasižymi didesne autonomine motyvacija, o autonominės motyvacijos teorija teigia, kad savikontrolės vykdymas turėtų būti efektyvesnis tiems, kurie turi savęs schemą. Remiantis tuo, šiame tyrime buvo tiriama, ar sveikai besimaitinančio savęs schemos statusas taip pat susilpnina savybinės savikontrolės ir sveikos mitybos elgesio ryšį, tokiu būdu, kad sumažina pirmojo poveikį antram. Šiame tyrime dalyvavo 149 žmonės. Tyrimas patvirtino sveikai besimaitinančio savęs schemą kaip moderatorių, t. y. parodė, kad sveikai besimaitinančio savęs schemos statusas susilpnina savybinės savikontrolės ir sveikos mitybos elgesio ryšį. Šis tyrimas galėtų būti naudingas asmenims, kurie turi problemų su savikontrolės reguliavimu ties sveika mityba.
Reikšminiai žodžiai: sveiko besimaitinančio savęs schemos būsena, savikontrolė, sveika mityba, jaunuoliai.
_________
Received: 10/01/2022. Accepted: 09/03/2022
Copyright © Justina Paluckaitė, 2022. Published by Vilnius University Press.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
A healthy diet reduces the risk of obesity and other health problems, such as hypertension, osteoporosis, colon cancer, and cardiovascular disease (Joshipura et al., 1999, 2001; Satia-Abouta, Galanko, Martin, Ammerman, Sandler, 2004; USDA and USDHHS Dietary Guidelines for Americans, 2010, as cited from Kendzierski et al, 2015). Importantly, dietary patterns that become stable as young people become fully independent eaters, not only have effects on their health but also continue into adulthood (Craigie et al., 2002; Craigie, Lake, Kelly, Adamson, Mathers, 2011; Mikkilä, Räsänen, Raitakari, Pietinen, Vikari, 2005, as cited from Kendzierski et al, 2015). While some individuals are successful at healthy eating, others struggle to maintain healthy diets. Most young people do not meet the recommended dietary guidelines, eating far too few fruits and vegetables and too much sugar and fat (Martinez-Gonzalez et al, 2011; Bingham et al, 2011; Pietinen et al, 2010, as cited from Hankonen et al, 2014). A range of psychological variables has been examined to explain these individual differences in eating behavior, since this might be helpful when tailoring interventions to promote healthy eating, and subsequently, a better overall health (Holub et al, 2012). Studies have demonstrated that trait level self-control, also referred to as trait self-control, is associated with a number of health behaviors, including healthy eating behavior (Hankonen, Kinnunen, Absetz, Jallinoja, 2014). Healthy eating behavior is associated with self-discipline and the need to exercise self-control to resist unhealthy foods (Bech-Larsen, Grunert, 2003; Koteyko, 2010; Niva, 2007, as cited from Barauskaite et al, 2018). Accordingly, people with high trait self-control eat more healthily as compared to those with low trait self-control (Hankonen et al, 2014).
Among other psychological variables, the concept of self-schema has become increasingly recognized for its role in regulating health behaviors, including in areas such as eating behavior (Kendzierski, 2007). Self-schema is a self-definition (i.e. self-identity), understood as being a domain-specific cognitive structure, originating from the past experiences of people, and which is concentrated on that aspect of the self which is considered by the individual as being important. Self-schema has two components: the first being self-description, which is domain specific, and the other being perceived importance attributed to that domain. Analogously, the healthy eater self-schema construct is also composed of two dimensions: self-description as a healthy eater and perceived importance of healthy eating. To have a healthy eater self-schema, individuals have to describe themselves as healthy eaters (i.e. self-description) and believe that healthy eating is important to the image they have of themselves (i.e. perceived importance) (Markus, 1977; Kendzierski, 1990; Kendzierski, Costello, 2004; Kendzierski, Whitaker, 1997). Some people can have a self-schema in the domain of, for example, healthy eating, while others might not have such schema at all. Also, within-person someone can have a schema for one specific domain, but not for its opposite (Kendzierski et al, 2015), e.g. for healthy eating as opposed to unhealthy eating. Schematics (those with a self-schema) have greater tendency to pay attention to information, which is schema-relevant, and interpret it as being such (Markus, 1977; Markus, Smith, Moreland, 1985, as cited from Kendzierski, Costello, 2004). Consistent with this, people who have a healthy eater self-schema status are more aware of, and receptive to the information about healthy eating and its issues. Such individuals are also more motivated to regulate their behavior in accordance with that information, and are more resilient to failures to do so (Kendzierski, Costello, 2004). Having a self-schema in a certain domain (e.g. healthy eating) also implies having more plans and strategies for doing schema-related behavior in that domain. Research has suggested that people who hold a specific self-schema are better at schema-related behaviors in this domain in comparison to those without such a self-schema. Moreover, self-perception as a healthy eater (i.e. having a healthy eater self-schema) predicted healthy eating intention and behavior in several studies (Kendzierski, Costello, 2004; Noureddine, Stein, 2009, as cited from Noureddine, Metzger, 2014). Those having a healthy eater self-schema, or at least describing themselves as such, make better food choices, experience less negative thoughts on food, and believe that challenges to eating healthily can be overcome (Holub et al, 2012). In other words, self-schemas are known to predict consistency of behaviors in healthy eating (Kendzierski, 1988, 1990). For example, previous research (Kendzierski, Costello, 2004; Noureddine, Stein, 2009) demonstrated that females who were healthy eater schematics reported consuming more nutritious diets than those who did not hold a healthy eater self-schema (i.e. were not schematic for healthy eating) (Holub et al, 2015).
The theory that supports this present research is the Theory of Self-Determination by Deci and Ryan (1985; 2000). Self-Determination Theory (SDT) is a macro theory which proposes an explanatory framework to predict self-regulated behavior (Deci, Ryan, 2008). It has been shown to be particularly relevant for eating behavior (Verstuyf et al., 2012). Central idea to SDT is that motivation can differ and be classified into two major categories: autonomous (self-determined) and controlled motivation. Controlled motivation happens when actions are driven by sources that are external to the actual behavior, e.g., avoidance of punishment, incentives, or perceived approval from others. This is also called External regulation. In contrast, autonomous motivation is more self-determined, and emanates from within oneself, from abiding values, or from personal interests (Deci, Ryan, 2000). Compared to controlled motivation, autonomous motivation has been shown to enhance performance and persistence in behavior. Identified regulation is a type of autonomous motivation that is driven by personal values or goals that individuals associate with a specific behavior. As regards a healthy diet, an apparent goal is to pursue ‘being healthy’. As a result of this process of identification, individuals approve and support their own behavior, and this has been shown to enhance commitment and performance (Deci, Ryan, 2000). Because more intrinsic types of autonomous motivation suggest that the actions are driven by pleasure or joy, and this might make it more complicated to digress from maintaining a healthy diet. Identified regulation is regarded as being particularly relevant to eating behavior (Verstuyf et al., 2012, as cited from De Man, Wouters, Delobelle, Puoane, Daivadanam, Absetz, Remmen, van Olmen, 2020).
While self-schemas are known to strengthen the link between intentions and behaviors (Kendzierski, 1988, 1990), and by itself implies having autonomous motivation to conduct an action, the trait self-control success relies on self-set goals that depend on autonomous motivation (Stavrova et al, 2019). Individual differences in self-control are associated with the extent to which an individual “wants to” pursue present-day goals. Some research suggests that self-control may also be especially effective for individuals with goals based on autonomous motivation (Erdvik, Øverby, Haugen, 2014; Sheldon, Elliot, 1999; Sheldon, Ryan, Deci, Kasser, 2004; Laran, Janiszewski, as cited from Converse et al, 2018) as opposed to goals that are pursued for controlled reasons (Laran, Janiszewski, 2011; Bénabóu, Tirole, 2003; Deci, Koestner, Ryan, 1999; Wrzesniewski et al., 2014, as cited from Converse et al, 2018). When people pursue goals for reasons that are autonomous, they tend to display sustained commitment. For example, resisting tempting chocolates is characterized by a lower self-control depletion when individuals report doing so because of internal, autonomous reasons (e.g. for an amusing challenge) as compared to external, controlled reasons (e.g. to make happy and satisfy the experimenter) (Muraven, 2008). Thus, autonomous motivation can also make self-control tasks less effortful (Masicampo et al, 2014). Most relevant to the current study, it was expected that the healthy eater self-schema could decrease the association between the trait self-control and healthy eating behavior. Because self-control to a large extent depends on how much an individual is determined to pursue one’s goals, having healthy eater self-schema status (having a self-schema in the domain of healthy eating, i.e. seeing oneself as a healthy eater) via autonomous motivation might strengthen goal commitment in the domain of healthy eating behavior. Thus, the theory of autonomous motivation (Deci, Ryan, 2000) implies that exercising self-control should be less necessary, i.e., require lower levels, for those schematic (those having a self-schema in the relevant domain), because autonomous motivation allows for voluntary actions that do not require excessive control and might compensate for the need to exert more self-control to achieve a result.
Because some people struggle to eat healthily, as a result of low self-control, this presupposes a pressing need for research regarding this matter. Previous studies have also stressed the importance of exercising self-control in healthy eating behavior, and have been investigating the possible ways by which the relationship is strengthened or hindered. However, the question of whether the healthy eater self-schema status affects the relation between trait self-control and healthy eating behavior has been never examined before. Facing the lack of research on this phenomenon, the present study formed a hypothesis that healthy eating self-schema status could be a moderator in the relation between trait self-control and healthy eating behavior. In other words, it was predicted that healthy eater self-schema status decreases the effect of trait self-control on healthy eating behavior.
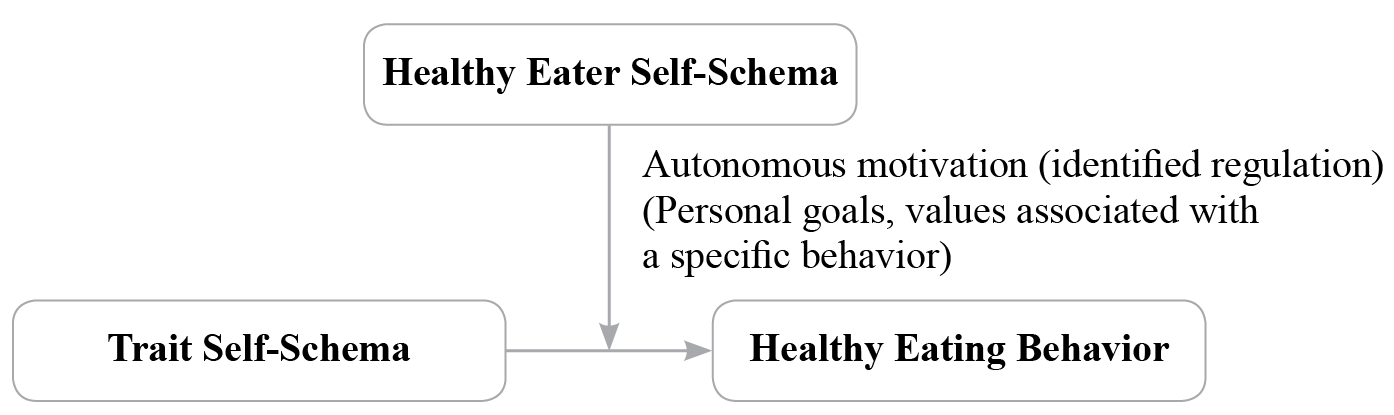
Figure 1. Conceptual moderation model
Compiled by the author of the article
Conceptual diagram of a simple moderation model (Fig. 1) in which the effect of the independent variable (trait self-control) on the dependent variable (healthy eating behavior) is influenced by the moderator (healthy eater self-schema).
Based on the above, the primary purpose of this study was to determine whether the healthy eater self-schema status decreased the relationship between trait self-control and healthy food consumption. Therefore, the following hypothesis was tested in the present paper: healthy eater self-schema status decreases the effect of trait self-control on healthy eating behavior. Additionally, the study also did several exploratory analyses. It examined associations between healthy eater schematics and other main variables of the study. No hypotheses were formed.
Research methodology
Method. Participants and Design
A total of 270 individuals submitted completed questionnaires. Four respondents were excluded from the analysis because they were schematic for unhealthy eating. These participants were eliminated from the study for several reasons. First, they comprised only a very small percentage of the sample, making it impossible to add it to further analyses. Moreover, recruiting a sufficient number of them would not have been feasible given the time and resources that were alloted to the present study. Second, these participants should not be grouped with healthy eater schematics because the content of their self-schema conceptually differs from that of healthy eater schematics. As a result, having a non-healthy eater self-schema would make it more problematic to adopt healthier eating behavior (Kendzierski et al, 2015). Third, these participants were eliminated from the analyses because the present study was only concerned with the prediction that having a healthy eater self-schema, in comparison to lacking that self-schema, promoted a weaker relationship between trait self-control and healthy eating behavior. In other words, unhealthy eater schematics (those who have a clear self-image as unhealthy eaters) were irrelevant, because the hypothesis focused only on healthy eater schematics and those who did not have a self-schema in this domain, and it was not the intent of the present study to see whether the type of self-schema mattered in the relationship between trait self-control and healthy eating behavior.
In addition, data from 74 participants was excluded because they did not complete the survey. 40 respondents who were over 30 years old were also excluded, because the present study was concerned only with risk group for unhealthy eating (young adults until the age of 30). Using SPSS statistics, tests were made on the trait self-control, healthy eater self-schema, healthy eating behavior and dieting variables to check for outliers and 7 participants were dropped out. Thus, the final sample consisted of 149 university students (109 female (73.2 %), 39 male (26.2 %), 1 both (.7%)) between the ages of 18 and 30 (M = 23.7, SD = 2.71; 55.7 % those with an undergraduate degree, 20.8 % those with a graduate degree, and 23.5 % other). The majority of participants were from the Netherlands (87.2 %), of these, 65 (43.6 % of the final sample) had a healthy eater self-schema, 84 (56.4 % of the final sample) had no self-schema in the domain. The design was cross-sectional.
Procedure
Participants were recruited using online questionnaires, which were distributed on the social networking site Facebook. Criteria for participation in the study was the following: being aged between 18 and 30 years old. To create the survey, Qualtrics online survey platform was used. Before starting the questionnaire, participants were asked to give an informed consent. A short description of the study was presented at the beginning of the survey. The questionnaire consisted of five parts, with the first three being designed to assess trait self-control tendencies, healthy eater self-schema status, and healthy eating behavior. In the final part, participants were asked to report demographic characteristics (age, gender, level of education (undergraduate, graduate, or other), and place of residence). Data was collected in 2020.
Materials
Trait self-control. Trait self-control was measured by the well-validated Trait Self-Control Scale (TSCS) (Tangney et al, 2004), designed to evaluate general self-control tendencies. The study employed the brief version of the scale, consisting of 13 items that were rated on a 7-point Likert scale (ranging from 1 (not at all) to 7 (very much)), such as “I am good at resisting temptation,” “I refuse things that are bad for me” and “I am able to work effectively toward long-term goals”. The short version was employed in order to reduce participant burden. The total score of the scale was used to assess the levels of trait-self control (Lindner et al, 2015). The 9 negatively phrased items were recoded in such a way that higher scores demonstrated higher levels of self-control. The scale has shown good reliability and validity (α = .85) (e.g. Malouf et al, 2014). In this study, Cronbach’s alpha was .86, which again indicated that the scale is highly reliable.
Healthy-Eater Self-Schema Status. The measure of the healthy eater self-schema status was Kendzierski and Costello’s (2004) Healthy Eating Self-Schema Scale (HESS) developed by Markus and colleagues to assess self-schema status (Catrambone, Markus, 1987; Markus, 1977; Markus, Smith, Moreland, 1985, as cited from Kendzierski et al, 2015). Participants were required to rate the self-descriptiveness of each of the three key phrases - healthy eater, someone who eats in a nutritious manner, and someone who is careful about what I eat. The items were assessed on an 11-point scale ranging from 1 (does not describe me) to 11 (describes me). They were also asked to rate the importance of additional three phrases - to the image you have of yourself, regardless of whether or not you are someone who is a healthy eater/who eats in a nutritious manner/who is careful about what you eat-on an 11-point scale varying from 1 (not at all important) to 11 (very important) (Kendzierski et al, 2015). The participants were categorized as healthy eater schematics if they rated at least two of the first three descriptive phrases as very self-descriptive (8-11 points on the 11-point scale) and two of the other three descriptive phrases as very important to their self-image (8-11 points on the 11-point scale). Participants who assessed at least two of the first three phrases as not very self-describing (1-4 points on the 11-point scale) and two of the other three phrases as having great importance (8-11 points on the 11-point scale) to their self-image, were categorized as being unhealthy eater schematics. All other participants were categorized as nonschematic for healthy eating (i.e., not having any self-schema in the domain of healthy eating - they neither see themselves as a healthy eater, nor as a non-healthy eater) (Kendzierski et al, 2015). The measure has demonstrated high internal consistency and reliability (α = .90) (e. g. Noureddine, Stein, 2009). Cronbach’s alpha for the scale was .65 in the current study (acceptable).
Healthy Eating Behavior. A 27-item self-reported Rate Your Plate food frequency questionnaire (Gans, 2000) was used to measure healthy food intake habits. It consists of questions which have focus on different categories of food and the frequency at which they are consumed. Each of the food items had three response options (with scores ranging from 1 to 3), with the third including the healthiest food options of the group. The total score of participants (with scores ranging from 27 to 81) is determined by the the sum of the item scores. Cronbach’s alpha in this present study was .79 (good).
Demographic information. Participants were asked to indicate their gender, age, level of education, and place of residence.
Data analysis
The data was analyzed by employing MS Excel 2016 and the IBM SPSS Statistics 20 computer program. All continuous variables were checked for normality. Data for the healthy eater self-schema variable was not normally distributed, except for the trait self-control and healthy eating behavior variables. Tests were made to check for outliers in scores for the main variables of interest in this study (healthy eater self-schema status, trait self-control, healthy eating behavior) and the other variables of secondary interest. To guarantee that assumptions of the level of measurement, related pairs, normality, linearity, multicollinearity, homoscedasticity, and independence of residuals were not violated, tests were done on the same main variables. Data was analysed using descriptive statistics, chi-square tests, bivariate associations, and a hierarchical multiple regression.
Results
Preliminary analyses
Using the method described previously, the participants were categorized as healthy eater self-schematics or nonschematics. Before investigating correlations between all psychological variables of the study (excluding place of residence), assumptions of normality, linearity and homeodascity were checked to ensure that they were not violated. No violations of the assumptions were found. Age was significantly positively related to the healthy eater self-schema, r(147) = .168, p = .043, while gender and education were not. Chi-square tests revealed that there were significant differences in the proportion of females and males who were classified as healthy eater schematics, χ2(1, N=149) = 1.38, p = .024.46.8 % of females were classified as healthy eater self-schematics, and 35.9 % of males were classified this way. Analyses (bivariate associations) indicated the healthy eater self-schema was significantly associated with the trait self-control and healthy eating, but not with the other variables of the study. There was a small, negative relationship between the two variables (r(14) = -.259, p = .048), with higher scores for the healthy eater self-schema associated with lower levels of trait self-control. A small, positive relationship between the healthy eater self-schema status and healthy eating behavior (r(147) = .180, p = .120), and a small, positive relationship between the healthy eating behavior and trait self-control (r(147) = .080, p = .341), were also found. In the current study, the mean scores for the main continuous variables of interest were the following: healthy eating behavior (M = 45.3; SD = 5.1); trait self-control (M = 40.7; SD = 4.6); healthy eater self-schema status (those having a healthy eater self-schema) (M = 30.9; SD = 5.2).
Primary analyses
Hierarchical multiple regression
A hierarchical multiple regression was used to perform moderation analysis. This is an appropriate method for moderation and is widely used in psychological research (Laerd Statistics, 2018). To ensure that the data can be analysed using hierarchical multiple regression, 8 assumptions were checked. No violations were observed. Control variables were not included in the analysis. Results of the hierarchical multiple regression indicated that the model explained 0.91 % of the variance and that the model was an insignificant predictor of the healthy eating behavior, F(1,197) = .276, p = .276. This indicated that there is potentially an insignificant moderation between trait self-control and healthy eater self-schema on healthy eating behavior.
Using the hierarchical multiple regression, the moderation analysis was performed to indicate if the healthy eater self-schema status moderated the association between trait self-control and healthy eating behavior. To avoid potentially problematic high multicollinearity with the interaction term, the variables were centered and an interaction term between trait self-control and healthy eater self-schema was created. Next, the interaction term between trait self-control and healthy eater self-schema was added to the regression model, which accounted for an insignificant proportion of the variance in healthy eating behavior, R2 = .091, F(1,197) = .276, p = .267, β = -.304, SE = .0181, t(35.719) = -.1.094, p = .276, CI [-.59, .017]. Examination of the interaction plot showed that there was an interaction effect between trait self-control and healthy eater self-schema on healthy eating behavior. The result was in line with the hypothesis (When the outliers were not eliminated, simple linear regression analyses suggested that there was potentially no significant moderation between trait self-control and healthy eater self-schema on healthy eating behavior).
Table 1. Regression analysis for predicting healthy eating behavior (N=149)
|
Variable |
B |
SE of B |
β |
t |
p |
|
Healthy eater self-schema Trait self-control |
-0.71 |
0181 |
-.304 |
-1.094 |
.276 |
Note: dependent variable healthy eating; R2 = .091, p = .276.
Discussion
This study examined whether the healthy eater self-schema status decreased the relationship between trait self-control and healthy eating behavior. A cross-sectional descriptive design was used to test the following hypothesis: (1) healthy eater self-schema status decreases the effect of trait self-control on healthy eating behavior. It was found that having a healthy eater self-schema status decreased the association between trait self-control and healthy eating behavior. The result was consistent with the hypothesis, which was based on the SDT theory of autonomous motivation (Deci, Ryan, 1985, 2000). There could be two possible reasons for such result.
First, SDT theory proposes that autonomous motivation evokes behaviors which are voluntary, are consistent with personal values, stem from peoples’ willingness and feel self-determined (Deci, Ryan, 2000). Healthy eater self-schema, which comprises autonomous motivation, and which regulates behavior by choice, based on personal importance and conscious valuing, enhances the commitment and performance of an individual in healthy eating, as well as increases persistence in behavior. This in turn might decrease the need to exert more self-control towards healthy eating. Resilience might be key in this process. The persistence in those having a self-schema is possibly due to the way how they perceive failures (Holub et, 2012). Because those schematic make attributions of failure in an irregular and even manner, they may anticipate more success in the future, which creates more motivation to persevere in the behavior. Believing that the lapses resulted from non-permanent obstacles increase the expectancy of future success and contribute to an increased motivation to persevere in healthy eating behaviors (Weiner, 1985; Swann, Rentfrow, & Guinn, 2003, as cited from Holub et al, 2012). For example, in a study by Kendzierski and Sheffield (2000) individuals with an exercise self-schema regarded the causes of the lapses as more short-term than those without such a self-schema, despite citing the same objective reasons for the lapses in their exercise behavior (Kendzierski, Sheffield, 2000). Thus, such resilience which is driven by autonomous motivation, and is inherent in healthy eater schematics, might compensate for the need to additionally exercise self-control in the relevant behavior.
Second, healthy eater self-schema, which is driven by SDT autonomous motivation, is linked to food preoccupation, which is an eating related cognition (Holub et al, 2012), and involves excessive or distracting thoughts about food. Healthy eater schematics have more overall positive food preoccupation, which includes having positive thoughts and associations with food. Positive cognitions about food possibly promote healthy eating behavior. Such preoccupation with food, a characteristic of healthy eater schematics (e.g. to continuously supporting focus on healthy food) may lead to self-control depletion, which in turn results in a lower capacity for self-control in healthy eating behavior. The Opportunity Cost Model theory argues that such depletion happens when the ongoing acts of self-control are no longer worth utilizing the mental processing power, resulting in the mental processes, which are capacity limited, being redirected to other activities (Inzlicht et al., 2014, Kurzban et al, 2013, as cited from Masicampo et al, 2014). Based on this theory, some of the mental processes, such as executive functions, working memory could be employed only to a limited number of tasks at a given time. Because self-control tasks occupy a greater portion of these mental processes compared to other, simpler tasks, when people exert self-control they cannot engage in other mental activities (Masicampo et al, 2014) (e.g., focusing on healthy foods, planning a healthy diet). Preoccupation with food in dieters was also characterized by an impaired cognitive performance, which most likely arises due to the depletion of accessible cognitive resources, as evidenced by one study (Jones, Rogers, 2003; Tapper, Pothos, 2010, as cited from Holub et al, 2012).
A limitation to the present study was that the participants of the study were volunteers from the social networking site Facebook, who were highly interested in the research topic, thus was subject to sampling bias, and this might have reduced the validity of results. It is clearly an empirical question whether findings from this sample could be generalized beyond those actually studied (e.g. middle aged). Further studies could address and clarify the issue. Another limitation of the study is its sample size. However, more participants could not have been recruited given the time and resources allotted to the study. For this reason, future studies are needed to determine the research question using a larger sample. Moreover, a common issue in using questionnaires is the impact of social desirability bias, when people respond in a way that is more socially acceptable. It would be recommended to use social desirability scales as control variables in future studies to enhance internal validity.
Future research could investigate the contributions of the separate healthy eater self-description and perceived importance dimensions, rather than simply investigating these components to classify people as self-schematics (Masicampo et al, 2014). Research is needed to examine the healthy eater self-schema in relation to other psychological self-constructs, especially across gender. It could also be explored whether healthy eater self-schema status is related with risk of eating disorders and later development of eating disorders (Holub et al, 2012).
Conclusion
The study provided evidence that self-description as a healthy eater and perceived importance attached to healthy eating do not play a role in the exercising of trait self-control towards healthy food consumption. Altogether, current results added to the expanding literature on the healthy eater self-schema’s role in the healthy eating behavior. This research contributed to a growing literature on the healthy eater self-schema, trait self-control and healthy eating behavior as well as enhanced the understanding of the relationships between them. The results of the study could benefit people with problematic eating behaviors. In addition, the investigation provided insights as to how best to tailor interventions aimed at improving eating behaviors and their management in individuals. Such study could also be helpful in tailoring future self-control interventions for individuals who have difficulties in exercising self-control toward healthy food consumption.
Acknowledgements
This article is partly based on my master thesis at Utrecht University. Data was collected in cooperation with Inger Wieringa.
I would like to thank to anonymous referees for their useful comments.
References
- Barauskaite, D., Gineikiene, J., Fennis, B. M., Auruskeviciene, V., Yamaguchi, M., Kondo, N. (2018). Eating healthy to impress: How conspicuous consumption, perceived self-control motivation, and descriptive normative influence determine functional food choices. Appetite, 131, 59–67. doi:10.1016/j.appet.2018.08.015
- Converse, B. A., Juarez, L., Hennecke, M. (2019). Self-control and the Reasons Behind Our Goals. Journal of Personality and Social Psychology: Personality Processes and Individual Differences, 116(15), 860-883.
- De Man, J., Wouters, E., Delobelle, P., Puoane, T., Daivadanam, M., Absetz, P., Remmen, R., van Olmen, J. (2020). Testing a Self-Determination Theory Model of Healthy Eating in a South African Township. Frontiers in Psychology, 11 (2181). doi: 10.3389/fpsyg.2020.02181
- Deci, E. L., Ryan, R. M. (1985). Intrinsic motivation and self-determination in human behavior. New York: Plenum.
- Deci, E. L., Ryan, R. M. (2000). The “What” and “Why” of goal pursuits: human needs and the self-determination of behavior. Psychol. Inquiry 11, 227–268. doi: 10.1207/s15327965pli1104_01
- Deci, E. L., Ryan, R. M. (2008). Self-determination theory: A macro theory of human motivation, development, and health. Canadian Psychology/Psychologie canadienne, 49(3), 182–185. https://doi.org/10.1037/a0012801
- Hankonen, N., Kinnunen, M., Absetz, P., Jallinoja, P. (2014). Why Do People High in Self-Control Eat More Healthily? Social Cognitions as Mediators. Annals of Behavioral Medicine, 47, 242–248. doi:10.1007/s12160-013-9535-1
- Holub, Sh. C., Haney, A. M., Roelse, M. (2012). Deconstructing the Concept of the Healthy Eater Self-Schematic: Relations to Dietary Intake, Weight and Eating Cognitions. Eating Behavior, 13(2), 106-11. doi:10.1016/j.eatbeh.2012.01.004
- Kendzierski, D. (1988). Self-schemata and exercise. Basic and Applied Social Psychology, 9(1), 45–59. https://doi.org/10.1207/s15324834basp0901_4
- Kendzierski, D. (1990). Exercise self-schemata: Cognitive and behavioral correlates. Health Psychology, 9, 69–82.
- Kendzierski, D. (2007). A Self-schema Approach to Healthy Eating. Journal of American Psychiatric Nurse Association, 12(6), 350-357.
- Kendzierski, D., Costello, M. C. (2004). Healthy eating self-schema and nutrition behavior. Journal of Applied Social Psychology, 34(12), 2437-2451.
- Kendzierski, D., Ritter, R. L., Stump, T. K., Anglin, C. L. (2015). The effectiveness of an implementation intentions intervention for fruit and vegetable consumption as moderated by self-schema status. Appetite, 95, 228-238. http://dx.doi.org/10.1016/j.appet.2015.07.007
- Kendzierski, D., Sheffield, A. (2000). Self-schema and attributions for an exercise lapse. Basic & Applied Social Psychology, 22, 1–8.
- Kendzierski, D., Whitaker, D. (1997). The role of self-schema in linking intentions with behavior. Personality and Social Psychology Bulletin, 23, 139-147.
- Laerd Statistics. 2018.
- Malouf, E. T., Schaefer, K. E., Witt, E. A., Moore, K. E., Stuewig, J., Tangney, J. P. (2014). The Brief Self-Control Scale Predicts Jail Inmates’ Recidivism, Substance Dependence, and Post-Release Adjustment. Personality and Social Psychology Bulletin, 40(3), 334–347.
- Markus, H. (1977). Self-schemata and processing information about the self. Journal of Personality and Social Psychology, 35, 63–78.
- Masicampo, E. J., Martin, S. R., Anderson, R. A. (2014). Understanding and overcoming self-control depletion: understanding and overcoming depletion. Social and Personality Psychology Compass, 8, 638–649. doi:10.1111/spc3.12139
- Muraven, M. (2008). Autonomous self-control is less depleting. Journal of Research in Personality, 42(3), 763–770. doi:10.1016/j.jrp.2007.08.002
- Noureddine, S., Metzger, B. (2014). Do Health-Related Feared Possible Selves Motivate Healthy Eating? Health psychology research, 2(1), 1043. https://doi.org/10.4081/hpr.2014.1043
- Noureddine, S., Stein, K. (2009). Healthy-eater self-schema and dietary intake. Western Journal of Nursing Research, 31(2), 201-218. http://refhub.elsevier.com/S0195-6663(17)30638-4/sref68
- Stavrova, O., Pronk, T., Kokkoris, M. D. (2019). Choosing goals that express the true self: A novel mechanism of the effect of self-control on goal attainment. European Journal of Social Psychology, 49, 1329–1336. https://doi.org/10.1002/ejsp.2559
- Tangney, J. P., Baumeister, R. F., Boone, A. L. (2004). High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. Journal of Personality, 72, 271–324. doi:10.1111/j.0022-3506.2004.00263.x
- Verstuyf, J., Patrick, H., Vansteenkiste, M., Teixeira, P. J. (2012). Motivational dynamics of eating regulation: a self-determination theory perspective. International Journal of Behavioral Nutrition and Physical Activity, 9, 21. doi: 10.1186/1479-5868-9-21