Acta medica Lituanica ISSN 1392-0138 eISSN 2029-4174
2021. Online ahead of print DOI: https://doi.org/10.15388/Amed.2021.28.1.9
Current Recommendations for Airway Management Techniques in COVID-19 Patients without Respiratory Failure Undergoing General Anaesthesia: A Nonsystematic Literature Review
Milda Grigonytė
Faculty of Medicine, Vilnius University, Vilnius, Lithuania
Agnė Kraujelytė
Faculty of Medicine, Vilnius University, Vilnius, Lithuania
Elija Januškevičiūtė
Faculty of Medicine, Vilnius University, Vilnius, Lithuania
Giedrius Šėmys
Faculty of Medicine, Vilnius University, Vilnius, Lithuania
Greta Bružytė-Narkienė
Faculty of Medicine, Vilnius University, Vilnius, Lithuania
Centre of Anaesthesiology, Intensive Therapy and Pain Management, Faculty of Medicine, Vilnius University, Vilnius, Lithuania
Oresta Kriukelytė
Faculty of Medicine, Vilnius University, Vilnius, Lithuania
Centre of Anaesthesiology, Intensive Therapy and Pain Management, Faculty of Medicine, Vilnius University, Vilnius, Lithuania
Eglė Kontrimavičiūtė*
Centre of Anaesthesiology, Intensive Therapy and Pain Management, Faculty of Medicine, Vilnius University, Vilnius, Lithuania
Nomeda Rima Valevičienė
Department of Radiology, Nuclear Medicine and Medical Physics, Faculty of Medicine, Vilnius University, Vilnius, Lithuania
Summary. Background. Since severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) first emerged, many articles have been published on airway management for coronavirus disease 2019 (COVID-19) patients. However, there is a lack of clear and concise conceptual framework for working with infected patients without respiratory failure undergoing general anaesthesia compared to noninfected patients. The aim of this article is to review current literature data on new challenges for anaesthesia providers, compare standard airway management techniques protocols with new data, and discuss optimisation potential.
Materials and methods. Literature search was performed in Google Scholar and PubMed databases using these keywords and their combinations: anaesthesia, preoxygenation, airway management, difficult airway, SARS-CoV-2, COVID-19. The following nonsystematic review is based on a comprehensive literature search of available data, wherein 41 articles were chosen for detailed analysis. Summarised and analysed data are presented in the article.
Results. SARS-CoV-2 has unique implications for airway management techniques in patients without respiratory failure undergoing general anesthesia. Main differences with the standard practice include: institutional preparedness, team composition principles, necessary skills, equipment, drugs, intubation and extubation strategies. Failed or difficult intubation is managed with predominance of emergency front of neck access (FONA) due to increased aerosol generation.
Conclusions. Airway management techniques in COVID-19 patients without respiratory failure are more challenging than in noninfected patients undergoing general anaesthesia. Safe, accurate and swift actions avoid unnecessary time delay ensuring the best care for patients, and reduce risk of contamination for staff. Appropriate airway strategy, communication, minimisation of time for aerosol generating procedures and ramped-up position aid to achieve these goals. During the pandemic, updated available literature data may change clinical practice as new evidence emerges.
Keywords: anaesthesia, preoxygenation, airway management, difficult airway, SARS-CoV-2, COVID-19.
Dabartinės kvėpavimo takų valdymo technikų rekomendacijos COVID-19 pacientams be kvėpavimo nepakankamumo taikant bendrąją anesteziją: nesisteminė literatūros apžvalga
Santrauka. Įvadas. Nuo sunkaus ūminio kvėpavimo sindromo koronaviruso 2 (SARS-CoV-2) atsiradimo buvo publikuota daug straipsnių apie COVID-19 sergančių pacientų kvėpavimo takų valdymą. Tačiau vis dar trūksta aiškios ir glaustos darbo su infekuotais pacientais be kvėpavimo nepakankamumo taikant bendrąją anesteziją, palyginti su neinfekuotais pacientais, koncepcijos. Šio straipsnio tikslas – apžvelgti dabartinius literatūros duomenis apie naujus iššūkius, su kuriais susiduria gydytojai anesteziologai, palyginti standartinių kvėpavimo takų valdymo technikų protokolus su naujais duomenimis ir aptarti darbo optimizavimo galimybes.
Medžiaga ir metodai. Literatūros paieška buvo atlikta „Google Scholar“ ir „PubMed“ duomenų bazėse, vartojant šiuos raktinius žodžius ir jų derinius: anestezija, preoksigenacija, kvėpavimo takų valdymas, sunkūs kvėpavimo takai, SARS-CoV-2, COVID-19. Po peržiūros, pagrįstos prieinamų duomenų literatūros paieška, išsamiai analizei buvo pasirinktas 41 straipsnis. Apibendrinta ir išanalizuota medžiaga pateikiama šiame straipsnyje.
Rezultatai. SARS-CoV-2 turi unikalią reikšmę parenkant kvėpavimo takų valdymo techniką pacientams be kvėpavimo nepakankamumo taikant bendrąją anesteziją. Pagrindiniai skirtumai, palyginti su standartine praktika, apima: bendrą pasirengimą, komandos sudėties principus, reikalingus įgūdžius, įrangą, vaistus, intubacijos ir ekstubacijos strategijas. Nepavykusi ar sunki intubacija yra valdoma atliekant skubią priekinę kaklo prieigą (FONA) dėl padidėjusios aerozolių generavimo rizikos.
Išvados. COVID-19 pacientų, kuriems nėra kvėpavimo nepakankamumo, kvėpavimo takų valdymo technikos yra sudėtingesnės, palyginti su neinfekuotais pacientais, kuriems taikoma bendroji anestezija. Saugūs, tikslūs ir greiti veiksmai leidžia išvengti nereikalingo delsimo, užtikrinama geriausia pacientų priežiūra ir mažėja darbuotojų užsikrėtimo rizika. Tinkama kvėpavimo takų valdymo strategija, bendravimas komandoje, aerozolius generuojančių procedūrų trukmės mažinimas ir taikoma pakeltos galvos padėtis padeda pasiekti šiuos tikslus. Pandemijos metu atnaujinti turimi literatūros duomenys gali keisti klinikinę praktiką atsiradus naujų mokslo įrodymų.
Raktiniai žodžiai: anestezija, preoksigenacija, kvėpavimo takų valdymas, sudėtingi kvėpavimo takai, SARS-CoV-2, COVID-19.
* Corresponding author: Eglė Kontrimavičiūtė, Santariškių 2, LT-08661, Vilnius, Lithuania, E-mail: egle.kontrimaviciute@santa.lt
Received: 1812/2020. Revised: 25/01/2021. Accepted: 10/02/2021
Copyright © 2021 Milda Grigonytė, Agnė Kraujelytė, Elija Januškevičiūtė, Giedrius Šėmys, Greta Bružytė-Narkienė, Oresta Kriukelytė, Eglė Kontrimavičiūtė, Nomeda Rima Valevičienė. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
The number of coronavirus disease 2019 (COVID-19) cases are increasing worldwide due to human-to-human transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1].
The novel coronavirus is highly contagious therefore in just under a year many articles have been published on airway management strategies for infected patients due to high risk of viral transmission with reported incidence of infection being 1,07 % among surgical patients; in addition to this, transmission was reported to medical staff [2, 3]. Furthermore, this infection has a tendency of respiratory system involvement and progressive lung damage that results in even more challenging management of a patient in urgent surgical scenarios [4, 5]. These patients could be more susceptible to desaturation during apnea after anaesthetic induction due to pathophysiology of the COVID-19, therefore these patients require expert airway management techniques to ensure safety during anaesthesia [6]. However, there is a lack of clear and concise conceptual framework for anaesthesia providers working with SARS-CoV-2 positive patients without respiratory failure in comparison with noninfected patients. As the number of infected patients continues to mount, it becomes paramount to prepare operating theatre staff for the inevitable arrival of SARS-CoV-2 positive patients for urgent surgeries.
The aim of this article is to review current literature data on the new challenges anaesthesia providers face while working with SARS-CoV-2 infected patients without respiratory failure during aerosol-generating procedures of airway management with high risk of infection transmission, to compare the standard airway management and difficult airway protocols with new data in the literature during COVID-19 pandemic, and discuss optimisation potential ensuring the highest anti-infective safety standards while providing the best care for a patient.
Materials and methods
Literature search was performed in Google Scholar and PubMed databases using these keywords and their combinations: anaesthesia, preoxygenation, airway management, difficult airway, SARS-CoV-2, COVID-19. The following nonsystematic review is based on a comprehensive literature search of available data, wherein 41 articles were chosen for detailed analysis. In the article, data for infected patients are summarised, analysed, and compared with those for noninfected patients.
A review of literature
Team
Preparation for airway management in SARS-CoV-2 positive patients brings new challenges to anaesthesia providers (Table 1).
Table 1. Preparation and plan before the procedure.
|
are |
Plan |
||||
|
Team |
Personal protective equipment (PPE) |
Equipment for endotracheal intubation |
Strategy |
Tracheal intubation checklist |
Use techniques you have tried before and used for other patients |
|
An experienced doctor for intubation; a second doctor specialist; an assistant to give medication and monitor patient‘s vital signs. |
Long sleeved gown; FFP3 mask; gloves; eyewear. |
COVID-19 intubation trolley. |
Preparation for routine intubation and for complicated intubation; all team members must be aware of procedure principles. |
This list can help to reduce the risk of human errors during preparation for endotracheal intubation. |
2-person 2-handed mask ventilation with a videolaryngoscopy is recommended. |
Preparation for the procedure begins outside the operating theatre door: composition of the team consists of two doctors anaesthesiologists and an assistant, dressed in a full personal protective equipment (PPE) with double gloves, defog goggles and/or eyewear [7]. A checklist for routine and difficult intubation in SARS-CoV-2 infected patients should be presented and discussed; the checklist allows to follow an action plan if the intubation does not proceed as expected and further actions must be taken without confusion [2]. The team should choose the airway devices that they are most familiar with. Intubation should be performed by the most experienced airway manager [8, 9]. If the intubation fails on the first attempt, the other qualified physician can take over the procedure. A runner should be outside the operating theatre and be able to provide help rapidly if needed [10].
We take this new literature data into consideration and emphasise a need for specialised training for hospital staff to ensure smooth coordinated efforts and teamwork.
Equipment
There are several differences in the equipment used in infected patients’ preoxygenation and endotracheal intubation in comparison with standard airway management. A separate COVID-19 intubation trolley should be prepared with the equipment required to intubate a patient safely, and brought into the operating theatre. The standard airway management trolley should also be kept outside the room; disposable single-use equipment should be used whenever possible [6]. The content of the COVID-19 trolley is similar to a standard difficult airway trolley, but there are some notable additions: at least 4 sets of PPE, a disposable Mapleson C circuit, and viral filters [7]. It is particularly important to attach a viral filter between the face mask and the anaesthetic circuit in order to avoid contamination of the circuit and contaminated gas expelling in the event of circuit disconnection [6]. Two filters (heat and moisture exchangers) should be fitted: one between the face mask and the elbow connector, and another at the expiratory limb of the anaesthetic circuit [2]. At least two laryngoscopes should be included in the set: a Macintosh direct laryngoscope and a Macintosh videolaryngoscope. As well as a hyperangulated videolaryngoscope should be included if available [6]. Due to fewer permissible failed intubations when performed by the most experienced airway manager in the team, videolaryngoscopy is a method of choice in COVID-19 patients [11]. Moreover, accurate, swift and safe intubation with videolaryngoscope helps to prevent episodes of desaturation, and doubles the distance between patient and operator faces [6, 12]. Wide range of endotracheal tubes (ETT), with preference of 7.0–7.5 mm ID for women and 8.0–9.0 mm ID for men, and the second generation supraglottic devices should be available [13, 14].
Drugs
Several alternative sedative agents are used in COVID-19 patients. Ketamine is a drug of choice for induction of anaesthesia with a dose of 0.5–2 mg/kg administered intravenously; doses should be considered individually for patients with heart disease [15, 16]. In hypoxic and agitated patients with difficult uptake of oxygen during preoxygenation, it is advisable to reassure the patient with a lower dose of ketamine (0.5 mg/kg) than is normally given during rapid induction. This dose does not inhibit respiratory activity and the quality of spontaneous ventilation, patients are more tolerant of a sealed mask, thus increasing the amount of oxygen supplied and reducing the risk of spreading viruses in the air. When preoxygenation is complete, rapid induction is performed using the remaining dose of ketamine [17]. Bronchodilation, due to sympathomimetic effects of ketamine, can also benefit to improve lung function and reduce airway resistance. Due to safer effects on the heart compared to ketamine, etomidate can be another drug of choice; an intravenous dose ranges 0.1–0.3 mg/kg [18]. Etomidate affects respiratory function: coughing may occur, which increases the chance of the virus spreading. Due to rapid onset and haemodynamic profile, midazolam can be an alternative sedative agent; an intravenous dose is 0.02–0.03 mg/kg. At high doses, midazolam may reduce systemic vascular resistance. Propofol should be avoided in hypotensive patients [15].
The most commonly used opioid in COVID-19 patients during induction is fentanyl with a dose of 0.5 to 3 mcg/kg administered intravenously [19]. Alternative opioids (like remifentanil) could also be used due to a little effect on haemodynamics. However, at higher doses, opioids may inhibit the myocardium and hypotension may occur due to the release of histamine. In addition to this, histamine can cause bronchospasm and chest wall muscle rigidity, making ventilation and oxygen saturation difficult [15].
The choice of neuromuscular blocking agents for these patients remains unclear. Rocuronium (0.6–1.2 mg/kg), vecuronium (0.08–0.1 mg/kg) or succinylcholine (0.3–1.1 mg/kg) are recommended [20, 21]. Succinylcholine, due to release of histamine, can cause bronchoconstriction, and may have a greater effect on the cardiovascular system compared to rocuronium and vecuronium [15].
COVID-19 patients may require infusion of a vasopressor (e.g. norepinephrine), what is more, some patients at high risk of haemodynamic decompensation may require an intravenous push-dose pressor (e.g. phenylephrine 100–200 mcg) [17].
Salbutamol may be administered to minimise airway resistance in patients with reactive airway disease [22]. Available current literature does not provide the most optimal salbutamol form and route of administration. For sudden breathing difficulties we suggest using the patient’ personal salbutamol pressurised metered-dose inhaler (pMDI) before and after anesthesia, or starting perioperative intravenous salbutamol infusion in order to decrease the risk of viral spreading.
Drugs, such as remifentanil, lidocaine, and dexmedetomidine, reduce the risk of coughing and minimise agitation on extubation [23]. Administration of intravenous lidocaine prior to tracheal extubation can effectively reduce emergence coughing without any other significant side effects. Consideration should be given to injections of lidocaine at the beginning and the end of any procedure requiring intubation and/or extubation in patients with COVID-19 [24].
Patient
Positioning
Current literature data distinguish two main patient positions: 45° head up or ramped-up position (Fig. 1) [25, 26, 27, 28]. These positions are important for high risk patients (obese, hypoxaemic and critically ill) because they facilitate face mask ventilation, laryngoscopy and intubation, delaying the onset of hypoxia [25, 26].
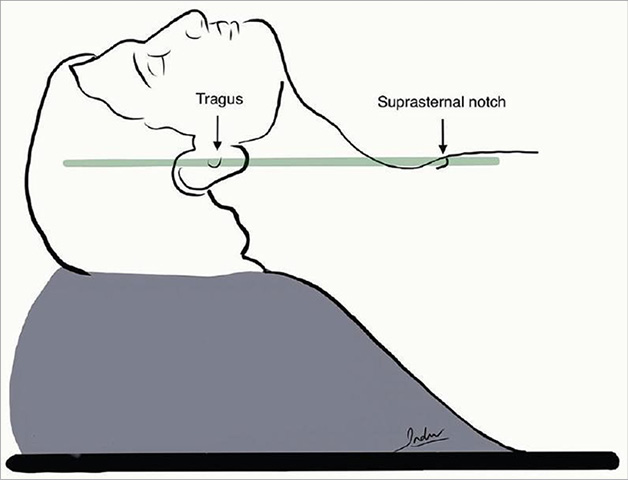
Fig. 1. Ramped-up position.
Preoxygenation, face mask ventilation and endotracheal intubation
In noninfected patients spontaneous ventilation is maintained by supplying pure oxygen at a flow rate of 5 l/min for 2 to 5 min with the tight fitting face mask [29, 30]. The delay between the onset of apnoea and the occurrence of arterial oxygen desaturation (SpO2 90%) is limited to 1–2 minutes and can be extended to 6–8 min with pre-oxygenation in 100% inhaled oxygen [25, 29, 30]. End-tidal oxygen fraction 90% should be accomplished with eight deep breaths at an oxygen flow of 10 l/min within 1 min including noninvasive ventilation [25, 26, 27, 29, 30, 31, 32]. Nasal oxygenation is also useful in securing a tube when needed to extend the apnoea time in difficult intubation. Furthermore, apnoenic oxygenation, in addition to standard preoxygenation and face mask ventilation, is useful in high-risk patients and in healthy patients [25, 26]. Noninvasive positive pressure ventilation can be beneficial in hypoxic, obese or critically ill patients [31]. Intubation should be limited in maximum 2 attempts with direct laryngoscopy [29, 31, 32].
Due to aerosol-generating intervention, a completely sealed surgical mask and two layers of wet gauze covering the patient’s nose and mouth are also helpful. When endotracheal intubation is planned, two persons with 2-handed “vice grip” technique with 100 percent oxygen preoxygenation at a minimum of 5 min is mandatory [7, 10]. Two anaesthetic circuits have been advised: circle or a hand-held (eg. Mapleson C) with the minimum obligatory <= 6 l/min oxygen flow [2]. Similar to noninfected patients, a low-flow nasal oxygen therapy (flow rate <5 L/min) is helpful in patients at risk of hypoxia, in an attempt to extend the apnoea time [10, 29, 33]. High-flow nasal oxygenation is beneficial for a shorter intubation time and decreasing incidence of desaturation when compared with preoxygenation by face mask ventilation [33, 34]. Nevertheless, due to the high risk of aerosolization and virus transmission, we suggest to limit use of noninvasive ventilation and high-flow nasal oxygenation only in negative pressure rooms. The cuff should be inflated with air to a measured cuff pressure of 20–30 cm H2O in order to avoid cuff leak; if using high airway pressures, secure cuff pressure ≥ 5 cm H2O above peak inspiratory pressure and start ventilation only after cuff inflation [28]. Auscultation to ensure correct intubation may be inefficient due to wearing PPE, capnography curve appearance and return of Et carbon dioxide over several respiratory cycles is the golden standard. A second generation supraglottic airway with a preference for the second generation laryngeal mask airway that allows inserting an ETT assisted by fiberoptic bronchoscopy is a method of choice in the event of failed endotracheal intubation; though these devices do not completely seal the airway [13, 14].
Endotracheal extubation
The process of extubation in COVID-19 patients has several differences compared to the standard extubation sequence, and is designed to ensure the safety of operating theatre staff (Table 2) [35]. Only those directly involved should be present at the time of extubation [7]. Pre-extubation suction of oral secretions is important and a suction tube should be placed inside the patient’s mouth while removing the ETT [36]. Just before extubation an anaesthesia mask fitted with a plastic sheet draped over it is placed above the ETT and once the ETT is removed, the mask is sealed tightly over the patient’s mouth and nose [23, 36]. The plastic sheet serves as a physical barrier for droplets generated during extubation and it is removed once the patient is breathing and coughing has subsided [36]. Mechanical ventilation is stopped prior to extubation. Once a firm seal is established, the mask should be connected to a viral filter and then back to the anaesthetic circuit. When the face mask is no longer required, a nasal cannula should be inserted and a surgical face mask placed over the patient’s nose and mouth [23]. Coughing during extubation generates a significant amount of droplets and poses a risk of viral transmission to staff, therefore it’s advised to suppress the cough reflex by administering medications [37]. The use of protective barrier hood devices is an option, however, there is currently a lack of evidence for or against their use in extubation [38].
Table 2. Comparison of noninfected and COVID-19 infected patient airway management.
|
Noninfected patient |
New for working with |
|
|
Position |
• Classic ‘sniffing’ |
• 45° head up or ramped-up |
|
Preoxygenation |
• Desaturation (SpO2 90%) limited to 1–2 min, can be extended to 6–8 min with pre-oxygenation in 100% inhaled oxygen |
• Airway assessment without removing the patient’s surgical mask |
|
Face mask ventilation |
• Avoid if high risk of aspiration; |
• Avoid as aerosol generating procedure |
|
Endotracheal intubation |
• Maximum 2 attempts |
• Most experienced/skilled airway manager |
|
Extubation |
• Assess for possible high risk extubation |
• Place a suction tube inside the mouth |
Difficult airway management
Difficult airway management in noninfected patients in comparison with COVID-19 patients is based on the algorithmic approach according to difficult airway management.
There are some principles that are the same in working with both groups of patients. The initial tracheal intubation plan A is to adequately pre-oxygenate, perform a neuromuscular blockade, if necessary, do external laryngeal manipulation, intubate the patient, and further maintain oxygenation and anesthesia. If plan A is successful, an anesthesiologist must confirm tracheal intubation with capnography. In the event of failed intubation, the team must execute plan B. At plan B, a 2nd generation supraglottic airway device must be used with maximum 3 attempts. If plan B is failed, at plan C there is a possibility to use a face mask, including two person technique and adjuncts. The plan D is recommended to execute when the patient cannot be intubated and oxygenated. In the emergent front of neck access case, it is important to ensure neuromuscular blockade, position the patient in order to extend neck and perform a procedure [7, 39]. Comparison of differences in techniques for noninfected and COVID-19 patients’ difficult airway management is presented in Table 3.
Cricothyroidotomy
Failed or difficult intubation is managed according to standard airway rescue algorithms with predominance of emergency front of neck access (FONA) due to risk of increased aerosol generation. Cricothyroidotomy must be performed as soon as possible when the patient cannot be intubated and ventilated. Firstly, it is important to exclude oxygen failure and blocked circuit and to ensure that this is maintained throughout airway management. Surgical cricothyrotomy should be the first-line procedure for ensuring airway function in COVID-19 patients (Table 3, plan D) [7]. There are various techniques and the choice must be made by the anaesthesiologist performing the procedure according to his experience and the preferable method, but the scalpel-bougie-tube technique is preferred in COVID-19 patients due to the risk of aerosolization with the oxygen insufflation associated techniques. The needle method is not recommended due to a small caliber of the needle, and therefore this method does not provide adequate oxygenation and ventilation [40, 41]. On the other hand cricothyroidotomy is rarely performed by anaesthesiologists, resulting in a lack of practical skills, thus the most experienced airway manager should perform this procedure if necessary.
Table 3. Comparison of non-infected and COVID-19 patients difficult airway management.
|
Plan A: Face mask ventilation and tracheal intubation |
Plan B: Maintaining oxygenation: SAD*** insertion |
Plan C: Face mask ventilation |
Plan D: Emergency front of neck access |
Post-FONA care and follow up |
|
|
Noninfected patient |
• Optimise head and neck position |
• 2nd generation device recommended |
• If face mask ventilation possible, paralyse |
• Continue to give oxygen via upper airway |
• Postpone surgery unless immediately life threatening |
|
New for working with COVID-19 infected patient |
• Staff must use full checked PPE* and share plan for failure |
• Plan B/C: Rescue oxygenation |
• Exclude oxygen failure and blocked circuit |
• Closed tracheal suction |
|
*PPE – personal protective equipment; **FONA – emergency front of neck access in airway management; *** SAD – supraglottic airway device; ****CICO – can’t intubate, can’t oxygenate.
Discussion and conclusions
Adequate management of preoxygenation, endotracheal intubation and tracheal extubation in SARS-CoV-2 infected patients without respiratory failure for urgent surgery under general anaesthesia is more challenging than in noninfected patients. Safe, accurate and swift actions avoid unnecessary time delay for urgent surgery, ensure the best care for patients, and reduce risk of contamination for healthcare workers. Appropriate airway strategy, staff communication, minimisation of time for aerosol generating procedures and ramped-up position aid to achieve these goals.
There are some weaknesses in this nonsystematic review. Due to newly developed extremely contagious aerosol-generating manipulations for medical staff during preoxygenation, tracheal intubation and extubation episodes, a small number of recommendations (mostly institutional) limits the available data for review on this topic. Scientific literature data based on early evidence (less than 1 year of COVID-19 pandemic) and an absence of randomised controlled trials limit the possibility to choose a systematic review type of article. In this nonsystematic review article we focus on aerosol-generating procedures (preoxygenation, intubation of trachea and extubation, difficult tracheal intubation) techniques in patients without respiratory failure and compare these techniques with recommendations and routine practice in noninfected individuals. We do not discuss COVID‐19 patient’s mechanical ventilation strategies but rather we focus on airway management techniques. Challenges could be faced while ventilating COVID-19 patients during urgent surgery, especially in those with COVID-19 pneumonia, acute respiratory distress syndrome, and changed respiratory system mechanics resulting in impaired oxygenation and ventilation. However, patients with respiratory failure deserve attention and it will be the focus of the future article. We also do not discuss particularities managing morbidly obese, pregnant, eldery and pediatric patients.
During the pandemic, updated available literature data may change clinical practice as new evidence emerges.
Conflict of interest
The authors declare that they have no conflict of interest.
Literature
- Mortaz E, Tabarsi P, Varahram M, Folkerts G, Adcock IM. The Immune Response and Immunopathology of COVID-19. Front Immunol [Internet]. 2020 Aug 26 [cited 2020 Nov 29];11. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7479965/; doi: https://doi.org/10.3389/fimmu.2020.02037.
- Thiruvenkatarajan V, Wong DT, Kothandan H, Sekhar V, Adhikary SD, Currie J, et al. Airway Management in the Operating Room and Interventional Suites in Known or Suspected Coronavirus Disease 2019 Adult Patients: A Practical Review. Anesth Analg [Internet]. 2020 Jun 9 [cited 2020 Nov 29]; Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7288783/; doi: https://doi.org/10.1213/ANE.0000000000005043.
- Hou J, Wan X, Shen Q, Zhu J, Leng Y, Zhao B, et al. COVID-19 infection, a potential threat to surgical patients and staff? A retrospective cohort study. Int J Surg. 2020 Oct;82:172–8; doi: https://doi.org/10.1016/j.ijsu.2020.08.037.
- Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020 May;109:102433; doi: https://doi.org/10.1016/j.jaut.2020.102433.
- Jin Y, Yang H, Ji W, Wu W, Chen S, Zhang W, et al. Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses. 2020 27;12(4); doi: https://doi.org/10.3390/v12040372.
- Brewster DJ, Chrimes N, Do TB, Fraser K, Groombridge CJ, Higgs A, et al. Consensus statement: Safe Airway Society principles of airway management and tracheal intubation specific to the COVID‐19 adult patient group. Med J Aust. 2020 Jun;212(10):472–81; doi: https://doi.org/10.5694/mja2.50598.
- Cook TM, El‐Boghdadly K, McGuire B, McNarry AF, Patel A, Higgs A. Consensus guidelines for managing the airway in patients with COVID‐19. Anaesthesia. 2020 Jun;75(6):785–99; doi: https://doi.org/10.1111/anae.15054.
- Ahmad I, El‐Boghdadly K, Bhagrath R, Hodzovic I, McNarry AF, Mir F, et al. Difficult Airway Society guidelines for awake tracheal intubation (ATI) in adults. Anaesthesia. 2020 Apr;75(4):509–28; doi: https://doi.org/10.1111/anae.14904.
- Higgs A, McGrath BA, Goddard C, Rangasami J, Suntharalingam G, Gale R, et al. Guidelines for the management of tracheal intubation in critically ill adults. British Journal of Anaesthesia. 2018 Feb 1;120(2):323–52; doi: https://doi.org/10.1016/j.bja.2017.10.021.
- Chen X, Liu Y, Gong Y, Guo X, Zuo M, Li J, et al. Perioperative Management of Patients Infected with the Novel CoronavirusRecommendation from the Joint Task Force of the Chinese Society of Anesthesiology and the Chinese Association of Anesthesiologists. Anesthesiology. 2020 Jun 1;132(6):1307–16; doi: https://doi.org/10.1097/ALN.0000000000003301.
- Lewis SR, Butler AR, Parker J, Cook TM, Schofield-Robinson OJ, Smith AF. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation: a Cochrane Systematic Review. Br J Anaesth. 2017 Sep 1;119(3):369–83; doi: https://doi.org/10.1093/bja/aex228.
- Hall D, Steel A, Heij R, Eley A, Young P. Videolaryngoscopy increases ‘mouth-to-mouth’ distance compared with direct laryngoscopy. Anaesthesia. 2020;75(6):822–3; doi: https://doi.org/10.1111/anae.15047.
- Wong DT, Yang JJ, Mak HY, Jagannathan N. Use of intubation introducers through a supraglottic airway to facilitate tracheal intubation: a brief review. Can J Anesth/J Can Anesth. 2012 Jul 1;59(7):704–15; doi: https://doi.org/10.1007/s12630-012-9714-8.
- Brimacombe J. The advantages of the LMA over the tracheal tube or facemask: a meta-analysis. Can J Anaesth. 1995 Nov 1;42(11):1017–23; doi: https://doi.org/10.1007/BF03011075.
- Ghia S, Lazar M, Epstein J, Bhatt HV. “Anesthesia Stat” to Intubate a Coronavirus Disease 2019 (COVID-19) Patient: Implications for the Anesthesiologist. J Cardiothorac Vasc Anesth. 2020 Oct;34(10):2566–70; doi: https://doi.org/10.1053/j.jvca.2020.05.016.
- Ketamine: Drug information - UpToDate. Accessed December 15, 2020. https://www.uptodate.com/contents/ketamine-drug-information
- Tracheal intubation of COVID-19 patients outside the OR - UpToDate. Accessed December 15, 2020. https://www.uptodate.com/contents/image/print?imageKey=EM%2F127516
- Etomidate: Drug information - UpToDate. Accessed December 15, 2020. https://www.uptodate.com/contents/etomidate-drug-information/
- Fentanyl: Drug information - UpToDate. Accessed December 15, 2020. https://www.uptodate.com/contents/fentanyl-drug-information/
- Vecuronium: Drug information - UpToDate. Accessed December 15, 2020. https://www.uptodate.com/contents/vecuronium-drug-information/
- Ghatehorde NK, Regunath H. Intubation Endotracheal Tube Medications. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 [cited 2020 Dec 15]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK459276/
- D’Silva DF, McCulloch TJ, Lim JS, Smith SS, Carayannis D. Extubation of patients with COVID-19. Br J Anaesth. 2020 Jul;125(1):e192–5; doi: https://doi.org/10.1016/j.bja.2020.03.016.
- Aminnejad R, Salimi A, Saeidi M. Lidocaine during intubation and extubation in patients with coronavirus disease (COVID-19). Can J Anaesth. 2020 Mar 16;1; doi: https://doi.org/10.1007/s12630-020-01627-2.
- Frerk C, Mitchell VS, McNarry AF, Mendonca C, Bhagrath R, Patel A, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth. 2015 Dec;115(6):827–48; doi: https://doi.org/10.1093/bja/aev371.
- Myatra SN, Shah A, Kundra P, Patwa A, Ramkumar V, Divatia JV, et al. All India Difficult Airway Association 2016 guidelines for the management of unanticipated difficult tracheal intubation in adults. Indian J Anaesth. 2016 Dec;60(12):885–98; doi: https://doi.org/10.4103/0019-5049.195481.
- Jensen AG, Callesen T, Hagemo JS, Hreinsson K, Lund V, Nordmark J, et al. Scandinavian clinical practice guidelines on general anaesthesia for emergency situations. Acta Anaesthesiol Scand. 2010 Sep;54(8):922–50; doi: https://doi.org/10.1111/j.1399-6576.2010.02277.x.
- Wong P, Lim WY. Aligning difficult airway guidelines with the anesthetic COVID-19 guidelines to develop a COVID-19 difficult airway strategy: a narrative review. J Anesth. 2020 Jul 8;1–20; doi: https://doi.org/10.1007/s00540-020-02819-2.
- Langeron O, Bourgain J-L, Francon D, Amour J, Baillard C, Bouroche G, et al. Difficult intubation and extubation in adult anaesthesia. Anaesthesia Critical Care & Pain Medicine. 2018 Dec 1;37(6):639–51; https://doi.org/doi: 10.1016/j.accpm.2018.03.013.
- Bouroche G, Bourgain JL. Preoxygenation and general anesthesia: a review. Minerva Anestesiol 2015 August;81(8):910-20.
- Japanese Society of Anesthesiologists. JSA airway management guideline 2014: to improve the safety of induction of anesthesia. J Anesth. 2014 Aug;28(4):482–93; doi: https://doi.org/10.1007/s00540-014-1844-4.
- Piepho T, Cavus E, Noppens R, Byhahn C, Dörges V, Zwissler B, et al. S1 guidelines on airway management : Guideline of the German Society of Anesthesiology and Intensive Care Medicine. Anaesthesist. 2015 Dec;64 Suppl 1:27–40; doi: https://doi.org/10.1007/s00101-015-0109-4.
- Meng L, Qiu H, Wan L, Ai Y, Xue Z, Guo Q, et al. Intubation and Ventilation amid the COVID-19 Outbreak. Anesthesiology [Internet]. 2020 Apr 8 [cited 2020 Dec 2]; Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7155908/; doi: https://doi.org/10.1097/ALN.0000000000003296.
- Wu C-N, Xia L-Z, Li K-H, Ma W-H, Yu D-N, Qu B, et al. High-flow nasal-oxygenation-assisted fibreoptic tracheal intubation in critically ill patients with COVID-19 pneumonia: a prospective randomised controlled trial. Br J Anaesth. 2020 Jul;125(1):e166–8; doi: https://doi.org/10.1016/j.bja.2020.02.020.
- Popat M, Mitchell V, Dravid R, Patel A, Swampillai C, Higgs A. Difficult Airway Society Guidelines for the management of tracheal extubation. Anaesthesia. 2012;67(3):318–40; doi: https://doi.org/10.1111/j.1365-2044.2012.07075.x.
- Asenjo JF. Safer intubation and extubation of patients with COVID-19. Can J Anaesth. 2020 Apr 22;1–3; doi: https://doi.org/10.1007/s12630-020-01666-9.
- Tung A, Fergusson NA, Ng N, Hu V, Dormuth C, Griesdale DEG. Medications to reduce emergence coughing after general anaesthesia with tracheal intubation: a systematic review and network meta-analysis. British Journal of Anaesthesia. 2020 Apr 1;124(4):480–95; doi: https://doi.org/10.1016/j.bja.2019.12.041.
- Kangas-Dick AW, Swearingen B, Wan E, Chawla K, Wiesel O. Safe extubation during the COVID-19 pandemic. Respir Med. 2020;170:106038; doi: https://doi.org/10.1016/j.rmed.2020.106038.
- Difficult airway algorithms and checklists [Internet]. Critical Care Airway Management. [cited 2020 Dec 13]. Available from: https://www.ccam.net.au/handbook/difficult-airway-algorithms-and-checklists/
- Šifrer R, Urbančič J, Piazza C, van Weert S, García-Purriños F, Benedik J, et al. Emergent tracheostomy during the pandemic of COVID-19: Slovenian National Recommendations. Eur Arch Otorhinolaryngol [Internet]. 2020 Sep 5 [cited 2020 Dec 15]; doi: https://doi.org/10.1007/s00405-020-06318-8.
- Lima DS, Ribeiro Junior MF, Vieira-Jr HM, Campos T de, Saverio SD. Alternatives for establishing a surgical airway during the COVID-19 pandemic. Rev Col Bras Cir. 2020;47:e20202549; doi: https://doi.org/10.1590/0100-6991e-20202549